◒
Acromioclavicular Joint Injection
From WikiMSK
This article is still missing information.

| |
| Acromioclavicular Joint Injection | |
|---|---|
| Indication | diagnosis, arthropathy |
| Syringe | 3-5mL |
| Needle | 25g 16mm |
| Steroid | 10-40mg triamcinolone |
| Local | 0.75mL 2% |
| Volume | 1-2mL |
Anatomy
The ACJ is a small joint therefore the injected volume should reflect this i.e maximum 2mL.
Indications
- pain - arthropathy i.e. osteoarthritis
- diagnostic injection
Contraindications
- Absolute: anaphylaxis to contrast/ injectates, active local/ systemic infection
- Relative: bleeding diathesis, recent injection with steroid in same/other body parts, unable to remain still for the procedure, young age
Technique
- Equipment
- ultrasound machine, sterile probe cover and a skin marker (ultrasound)
- skin marker, a metal rod for marking and short connecting tube (fluoroscopy)
- skin cleaning product
- sterile drape
- sterile field and tray for sharps
- syringe selection i.e. 5mL and 3mL (US)
- larger bore drawing up needle
- needle to administer local anaesthetic i.e. 30 or 25-gauge needle
- needle to cannulate the joint i.e. 25 or 27-gauge needle
- injectants i.e. local anaesthetics, iodinated contrast, corticosteroid preparation
- sterile gauze
- adhesive dressing
Landmark Guided
Ultrasound Guided
Longitudinal
Transverse
Transverse


- In plane
- optimise patient positioning by lying them flat and supine on the bed for cranial access, or at 45 degrees for anterior access
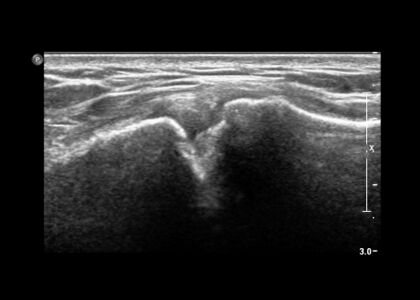
- identify ACJ in the transverse plane; perpendicular to the clavicle, and optimise imaging and mark skin entry point
- clean skin and draw up appropriate medications
- consider local anaesthesia along the proposed needle path
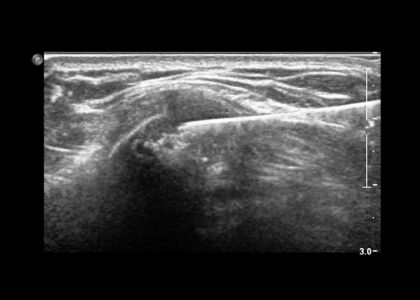
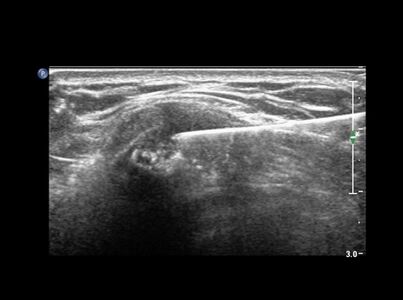
- under ultrasound guidance using anterior or cranial access, insert the needle in-plane with the probe into the ACJ
- administer arthrogram injectate under direct visualisation
- remove needle and apply dressing/ band-aid as required
- Out of plane
- optimise patient positioning by lying them flat and supine on the bed or at 45 degrees, the joint will be accessed cranially
- identify the ACJ in a longitudinal plane; parallel to the clavicle, with the ACJ in the centre of the image. Optimise imaging and mark skin at the probe midpoint
- clean skin and draw up appropriate medications
- consider local anaesthesia along the proposed needle path
- under ultrasound guidance using cranial access, insert the needle at the probe midpoint and out-of-plane with the probe into the ACJ
- administer arthrogram injectate
- remove needle and apply dressing/ band-aid as required
Fluoroscopy Guided
- optimise patient positioning by lying them supine on bed, the joint is accessed anteriorly
- optimise imaging field and using the metal rod, mark the skin at the target entry at the midpoint of the joint
- clean skin and draw up appropriate medications
- consider local anaesthesia along the proposed needle path
- under fluoroscopic guidance using anterior access, insert a needle into the ACJ
- check for an intra-articular needle tip position with a small amount of iodinated contrast via connection tubing and save a post injection image
- administer arthrogram injectate
- remove needle and apply dressing/ band-aid as required
Complications
Steroid flare is a relatively common side effect which will settle after 1 or 2 days. The most serious complication is infection causing septic arthritis. Steroid containing injections should be postponed if there are any signs and/or symptoms of local and/ or systemic infective. Fat necrosis causing skin dimpling and skin discolouration can occur due to steroid leaking into the surrounding soft tissues
Aftercare
Videos
External Links
References
Part or all of this article or section is derived from Acromioclavicular joint injection (technique) by Dr Dai Roberts et al., used under CC BY-NC-SA 3.0
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,

