Adult Acquired Flatfoot Deformity: Difference between revisions
No edit summary |
|||
| (11 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{partial}} | |||
[[File:Adult Acquired Flatfoot Radiograph.jpg|thumb|Adult Acquired Flatfoot Radiograph demonstrating AAFD with increased talar head uncoverage and forefoot abduction. Contributed by Mark A. Dreyer, DPM, FACFAS]] | [[File:Adult Acquired Flatfoot Radiograph.jpg|thumb|Adult Acquired Flatfoot Radiograph demonstrating AAFD with increased talar head uncoverage and forefoot abduction. Contributed by Mark A. Dreyer, DPM, FACFAS]] | ||
Adult acquired flatfoot (AAFD), formerly described as posterior tibial tendon dysfunction (PTTD) | Adult acquired flatfoot (AAFD), formerly described as posterior tibial tendon dysfunction (PTTD) has complex pathology defined by the collapse of the medial longitudinal arch of the foot with continued progressive deformity of the foot and ankle. <ref name=":0">Deland JT. Adult-acquired flatfoot deformity. J Am Acad Orthop Surg. 2008 Jul;16(7):399-406. [PubMed]</ref> | ||
== | == Anatomy == | ||
The anatomy of the foot and ankle are complex, with multiple structures involved in the stability and function needed to walk and bear weight. | |||
A structure principally involved in the development of adult acquired flatfoot is the posterior tibialis tendon. In addition to plantar flexion, the posterior tibialis tendon is the primary inverter of the foot. It inserts principally on the navicular tuberosity, but also has lesser insertions on to other tarsal and metatarsal structures.<ref name=":1">Abousayed MM, Alley MC, Shakked R, Rosenbaum AJ. Adult-Acquired Flatfoot Deformity: Etiology, Diagnosis, and Management. JBJS Rev. 2017 Aug;5(8):e7.</ref> | |||
The spring and deltoid ligaments are crucial to the stability of the foot and ankle. The spring ligament, which is the ligament most frequently involved in adult-acquired flatfoot, supports the ankle by connections from the sustentaculum tali of the calcaneus to the navicular. The primary role of the spring ligament is to support the head of the talus.<ref>Bastias GF, Dalmau-Pastor M, Astudillo C, Pellegrini MJ. Spring Ligament Instability. Foot Ankle Clin. 2018 Dec;23(4):659-678.</ref> The deltoid ligament is usually affected later in the progression of the adult acquired flatfoot. The superficial deltoid ligament has a wide insertion on the navicular to the posterior tibiotalar capsule. It is the primary support against tibiotalar valgus angulation. The deep deltoid ligament prevents axial rotation of the talus, where it inserts, from its origin on the intercollicular groove and posterior colliculus. The deltoid ligament as a whole is critical in supporting the articulating surfaces of the ankle and the spring ligament.<ref name=":2">Smith JT, Bluman EM. Update on stage IV acquired adult flatfoot disorder: when the deltoid ligament becomes dysfunctional. Foot Ankle Clin. 2012 Jun;17(2):351-60.</ref> | |||
== | ==Development== | ||
Acquired flatfoot was historically attributed to posterior tibial tendon deficiency, although now the understanding is that the ligamentous structures of the ankle play a role in adult-acquired flatfoot development. | All children are born with flat feet. Toddlers may walk with a flatfoot posture in order to have their feet resting entirely on the ground with their weight over the first or second tarsometatarsal joints. In most children the longitudinal arch develops by the time they are 10 years old. At this stage treatment is not indicated. However a full arch may not develop, and the persistence of physiological flexible flatfoot into adulthood is common. | ||
== Aetiology and Pathophysiology == | |||
Acquired flatfoot was historically attributed to posterior tibial tendon deficiency, although now the understanding is that the ligamentous structures of the ankle play a role in adult-acquired flatfoot development.<ref name=":0" /><ref name=":3">Abousayed MM, Tartaglione JP, Rosenbaum AJ, Dipreta JA. Classifications in Brief: Johnson and Strom Classification of Adult-acquired Flatfoot Deformity. Clin Orthop Relat Res. 2016 Feb;474(2):588-93.</ref> The dysfunction of the posterior tibial tendon is a multifactorial process. In many patients, there is a preexisting flatfoot, and many patients are also obese. Another factor is a relative hypovascularity of the tendon as it makes an abrupt turn posterior to the medial malleolus; this predisposes the tendon to rupture due to insufficient repair.<ref>Petersen W, Hohmann G, Stein V, Tillmann B. The blood supply of the posterior tibial tendon. J Bone Joint Surg Br. 2002 Jan;84(1):141-4</ref> Episodes of previous trauma, corticosteroid injections, arthritis, neuromuscular conditions, and diabetes all predispose to the development of an adult acquired flatfoot.<ref name=":5">Holmes GB, Mann RA. Possible epidemiological factors associated with rupture of the posterior tibial tendon. Foot Ankle. 1992 Feb;13(2):70-9</ref> | |||
The posterior tibial tendon is critical in maintaining the appropriate gait and function of the foot. Contraction of the tibialis posterior causes inversion of the foot and locking of the [[Transverse Tarsal Joint (Chopart's Joint)|transverse tarsal joints]] granting stability for push-off.<ref name=":1" /> Deficiency of the posterior tibialis tendon leads to an unstable transverse tarsal joint and forefoot abduction, allowing unopposed action of the peroneus brevis. The ensuing abduction of the forefoot and transverse talar joints also displaces the force of the calcaneal tendon laterally, further accentuating the valgus defect of the foot.<ref>Brodsky JW. Preliminary gait analysis results after posterior tibial tendon reconstruction: a prospective study. Foot Ankle Int. 2004 Feb;25(2):96-100</ref> The continued strain on the static stabilizing ligaments eventually leads to their attenuation. Most commonly, the spring ligament is affected, failure leads to medial and plantar subluxation of the talar head relative to the navicular. Failure of the deltoid ligament will lead to a valgus position of the talus within the ankle mortise.<ref name=":0" /><ref name=":1" /><ref name=":2" /><ref name=":4">Smyth NA, Aiyer AA, Kaplan JR, Carmody CA, Kadakia AR. Adult-acquired flatfoot deformity. Eur J Orthop Surg Traumatol. 2017 May;27(4):433-439</ref><ref name=":5" /> These events may occur in a stepwise fashion, corresponding to Johnson and Strom classification system. However, some patients develop a valgus talar tilt without a fixed flatfoot deformity.<ref name=":2" /> | |||
== Epidemiology == | == Epidemiology == | ||
Acquired flatfoot is a common | Acquired flatfoot is a common orthopaedic condition, although there is a relative paucity of literature on the epidemiology regarding adult acquired flatfoot. There are 5 million people in the United States affected with adult acquired flatfoot. In the UK, the estimated prevalence is estimated to be over 3% in women over 40 years old.<ref>Kohls-Gatzoulis J, Woods B, Angel JC, Singh D. The prevalence of symptomatic posterior tibialis tendon dysfunction in women over the age of 40 in England. Foot Ankle Surg. 2009;15(2):75-81.</ref> Posterior tibial tendon issues are prevalent in the geriatric population, with 10% of geriatric patients affected. The geriatric population might be predisposed to more severe adult acquired flatfoot due to the degeneration of muscle mass and bone structure, as well.<ref>Ikpeze TC, Brodell JD, Chen RE, Oh I. Evaluation and Treatment of Posterior Tibialis Tendon Insufficiency in the Elderly Patients. Geriatr Orthop Surg Rehabil. 2019;10:2151459318821461.</ref> Patients with chronic vascular diseases are at increased risk; this includes diabetics and patients with hypertension.<ref name=":5" /> | ||
== Classification == | |||
Acquired flatfoot grading is by the Johnson and Strom classification system, which has classification grades of I to III.<ref>Johnson KA, Strom DE. Tibialis posterior tendon dysfunction. Clin Orthop Relat Res. 1989 Feb;(239):196-206.</ref> Myerson added a fourth grade in 1997.<ref>Myerson MS. Adult acquired flatfoot deformity: treatment of dysfunction of the posterior tibial tendon. Instr Course Lect. 1997;46:393-405. </ref> The classification system aids practitioners in identifying AAFD severity and also can guide treatment plans.<ref name=":3" /> | |||
* Stage I: characteristically presents with posterior tibial tendon tenosynovitis with no arch collapse. | |||
* Stage II: foot collapse and will be unable to perform a single-leg heel rise. | |||
** Stage IIa: foot collapse with valgus deformity of the hindfoot but no midfoot abduction | |||
** Stage IIb: midfoot abduction is present. | |||
* Stage III: fixed deformity with hindfoot valgus and forefoot abduction. | |||
* Stage IV: ankle valgus secondary to deltoid ligament attenuation.<ref name=":4" /> | |||
== | == Assessment == | ||
It is essential to evaluate the patient with suspected adult acquired flatfoot during weight-bearing. There are specific hallmark findings of adult acquired flatfoot for which practitioners should look. While the patient is standing with the provider behind excessive abduction of the forefoot can be noted by the “too many toes” sign. This test is positive if the practitioner can see more than the fifth and part of the fourth toe. Inspection and palpation over the posterior tibial tendon at the area of the medial malleolus may demonstrate swelling or pain. On the lateral aspect of the foot pain may be elicited if there is impingement of ligamentous structures. | It is essential to evaluate the patient with suspected adult acquired flatfoot during weight-bearing. There are specific hallmark findings of adult acquired flatfoot for which practitioners should look. While the patient is standing with the provider behind excessive abduction of the forefoot can be noted by the “too many toes” sign. This test is positive if the practitioner can see more than the fifth and part of the fourth toe. Inspection and palpation over the posterior tibial tendon at the area of the medial malleolus may demonstrate swelling or pain. On the lateral aspect of the foot pain may be elicited if there is impingement of ligamentous structures.<ref name=":6">Vulcano E, Deland JT, Ellis SJ. Approach and treatment of the adult acquired flatfoot deformity. Curr Rev Musculoskelet Med. 2013 Dec;6(4):294-303</ref> Single and double heel rise tests may be performed to assess the strength of the posterior tibial tendon. Failure to invert the foot on heel rise or perform heel rise at all is considered indicative of posterior tibial tendon dysfunction. Ankle range of motion requires assessment. Effort should be made to correct valgus deformity in a range of motion exercise to evaluate for fixed deformity. A fixed deformity of the subtalar joint or fixed abduction of the forefoot has implications in treatment.<ref name=":1" /> | ||
= | {| class="wikitable" | ||
|+Acquired Flat Foot Classification with Clinical Features, Pathology, and Imaging Findings | |||
!Stage | |||
!Clinical Features | |||
!Pathology | |||
!Imaging | |||
|- | |||
|I | |||
| | |||
* Medial pain and swelling | |||
* Single limb heel rise positive | |||
* No arch collapse | |||
| | |||
* Normal tendon length | |||
* Tenosynovitis | |||
| | |||
* MRI/USS: tenosynovitis | |||
|- | |||
|IIA | |||
| | |||
* Obvious but flexible deformity | |||
* Medial pain and swelling | |||
* Single limb heel rise positive | |||
* Too many toes sign positive | |||
| | |||
* Tendon elongation | |||
* Tenosynovitis | |||
* Flatfoot deformity | |||
| | |||
* Xray: uncovering talar head | |||
* MRI/USS: tenosynovitis, splits | |||
|- | |||
|IIB | |||
| | |||
* Obvious deformity | |||
* Medial and lateral pain | |||
* Single limb heel rise negative | |||
* Too many toes sign positive | |||
| | |||
* Tendon elongation | |||
* Degenerative changes | |||
* Lateral impingement | |||
| | |||
* Xray: OA | |||
* MRI: soft tissue changes | |||
|- | |||
|III | |||
| | |||
* Rigid valgus deformity, forefoot varus >15° | |||
* Tight tendo-Achilles | |||
* Lateral pain | |||
* Pain at rest | |||
| | |||
* Subtalar OA | |||
* Lateral impingement | |||
| | |||
* Xray: OA | |||
* MRI: soft tissue changes | |||
|- | |||
|IV | |||
| | |||
* Lateral ankle pain | |||
* Rigid deformity | |||
| | |||
* Advanced OA, now also in ankle | |||
| | |||
* Xray: OA | |||
* MRI: soft tissue changes | |||
|} | |||
== Differential Diagnosis == | |||
While the diagnosis of adult acquired flatfoot is relatively straightforward, the following differentials should be considered. A careful history and physical examination can usually rule out most of these conditions.<ref>Lee MS, Vanore JV, Thomas JL, Catanzariti AR, Kogler G, Kravitz SR, Miller SJ, Gassen SC., Clinical Practice Guideline Adult Flatfoot Panel. Diagnosis and treatment of adult flatfoot. J Foot Ankle Surg. 2005 Mar-Apr;44(2):78-113</ref> | |||
{{DDX Box|ddx-title=Adult Acquired Foot Differential Diagnosis|ddx-text= | |||
*Flexible, Non-PTTD (physiological from childhood) | |||
*Flexible, PTTD (flexible unless severe) | |||
*Structural (tarsal coalition, accessory navicular) | |||
*Inflammatory (RhA, Spondyloarthropathies) | |||
*Degenerative | |||
*Neurological (cerebral palsy) | |||
*Post traumatic}} | |||
== Imaging == | |||
The gold standard for the evaluation of adult acquired flatfoot is weight-bearing radiographs. Radiographs are necessary in the anteroposterior, lateral, and hindfoot views. These views will assess the degree of arch collapse, particularly by measuring the lateral first tarsometatarsal angle, and forefoot abduction at the talonavicular joint. Talar head uncoverage can also be measured in the setting of stage IV disease by the lateral talonavicular angle. Lateral views of the foot can also display naviculocuneiform and first tarsometatarsal collapse. Arthritis should be carefully assessed on all radiographic films as this may have implications on treatment options.<ref name=":6" /> | |||
== | MRI is typically not needed for evaluation of adult acquired flatfoot; however, it may be beneficial for some patients with ligamentous involvement that may alter surgical treatment planning; this is particularly relevant for patients with medial peritalar instability, who have improved functional outcomes with deltoid-spring ligament reconstruction.<ref>Brodell JD, MacDonald A, Perkins JA, Deland JT, Oh I. Deltoid-Spring Ligament Reconstruction in Adult Acquired Flatfoot Deformity With Medial Peritalar Instability. Foot Ankle Int. 2019 Jul;40(7):753-761.</ref> | ||
Several studies indicate that ultrasound may be a useful modality in assessing the posterior tibial tendon when compared to the more time consuming and costly MRI. Results from an ultrasonographic evaluation of the posterior tibial tendon were equivalent to MRI in 87% to 94% of patients.<ref>Arnoldner MA, Gruber M, Syré S, Kristen KH, Trnka HJ, Kainberger F, Bodner G. Imaging of posterior tibial tendon dysfunction--Comparison of high-resolution ultrasound and 3T MRI. Eur J Radiol. 2015 Sep;84(9):1777-81</ref><ref>Harish S, Kumbhare D, O'Neill J, Popowich T. Comparison of sonography and magnetic resonance imaging for spring ligament abnormalities: preliminary study. J Ultrasound Med. 2008 Aug;27(8):1145-52</ref> | |||
===Imaging Case=== | |||
44 year old man with two year history of relapsing medial ankle pain. On exam has hindfoot valgus with medial arch collapse and tenderness over the medial column. Xray showed planovalgus foot with pes planus 20 degrees and hindfoot valgus 32 degrees. No significant radiographic osteoarthritis. Ultrasound showed the tibialis posterior tendon sheath to be very thickened with considerable adjacent vascularity. The tendon itself remained intact. Corticosteroid injection, orthotics, and a graded exercise programme were orgnaised. | |||
<gallery> | |||
File:AAFFD xray AP.jpg|AP xray | |||
File:AAFFD xray lateral.jpg|Lateral xray | |||
File:AAFFD xray mortise.jpg|Mortise xray | |||
File:AAFFD xray weightbearing.jpg|Weightberaing foot xray | |||
File:AAFFD xray weightbearing 2.jpg|Weightbearing foot xray | |||
File:AAFD_tibialis_posterior_tenosynovitis.jpg|Tibialis posterior tenosynovitis | |||
</gallery> | |||
== Management == | |||
The treatment of adult acquired flatfoot is complex. There are multiple treatment options, and the treatment of adult-acquired flatfoot has been the focus of most recent research. However, first-line therapy for the condition remains nonoperative. | The treatment of adult acquired flatfoot is complex. There are multiple treatment options, and the treatment of adult-acquired flatfoot has been the focus of most recent research. However, first-line therapy for the condition remains nonoperative. | ||
Treatment with orthotic devices, such as low-articulating ankle-foot orthosis, cast-boot walkers, and other ankle-foot orthoses in conjunction with NSAID therapy and physical therapy have a resolution of symptoms 87% of the time according to one study. Other studies have success rates of 67 to 90% with conservative measures. | === Non-operative === | ||
Treatment with orthotic devices, such as low-articulating ankle-foot orthosis, cast-boot walkers, and other ankle-foot orthoses in conjunction with NSAID therapy and physical therapy have a resolution of symptoms 87% of the time according to one study. Other studies have success rates of 67 to 90% with conservative measures.<ref name=":6" /> | |||
Acquired flatfoot appears to be associated with obesity, diabetes, hypertension, and other disease processes that are treatable with a healthy lifestyle and weight reduction. Patients with adult acquired flatfoot may benefit from the treatment of their other medical comorbidities. Additionally, patients may prevent further disease progression once diagnosed with the use of an appropriate orthotic device. Most patients who use an orthotic device in conjunction with PT and or NSAID therapy will not need any surgical intervention.<ref name=":6" /> | |||
=== Surgery === | |||
Surgical treatment is indicated in patients who have attempted conservative therapy and are not satisfied with their results. Surgical treatment depends on the stage of the disease, as well as other factors including medical comorbidities, functional status, and use of tobacco. | Surgical treatment is indicated in patients who have attempted conservative therapy and are not satisfied with their results. Surgical treatment depends on the stage of the disease, as well as other factors including medical comorbidities, functional status, and use of tobacco. | ||
Surgical management of stage I disease is uncommon, but if required patients should undergo posterior tibial tendon tenosynovectomy, debridement, or flexor digitorum longus tendon autograft. There is a concern that repair of the posterior tibial tendon may experience complications with long-term failure; therefore, surgical treatment should be carefully considered prior to any intervention. | Surgical management of stage I disease is uncommon, but if required patients should undergo posterior tibial tendon tenosynovectomy, debridement, or flexor digitorum longus tendon autograft. There is a concern that repair of the posterior tibial tendon may experience complications with long-term failure; therefore, surgical treatment should be carefully considered prior to any intervention.<ref name=":4" /> | ||
Stage | Stage II disease treatment has been successful by medializing calcaneal osteotomy in addition to a flexor digitorum longus transfer. One study showed 87% of patient satisfaction with this treatment after a mean follow-up of 15 years.<ref>Chadwick C, Whitehouse SL, Saxby TS. Long-term follow-up of flexor digitorum longus transfer and calcaneal osteotomy for stage II posterior tibial tendon dysfunction. Bone Joint J. 2015 Mar;97-B(3):346-52</ref> | ||
Stage | Stage III disease becomes more challenging to treat due to the fixed nature of the defect. Arthrodesis is the standard of care, with double and triple arthrodesis being common. Double arthrodesis entails a fusion of the subtalar and talonavicular joints. Triple arthrodesis involves the calcaneocuboid joint in addition to the two joints mentioned above. Double arthrodesis has the advantage of reduced arthritic complications and reduced joint stiffness associated with calcaneocuboid fusion. Unfortunately, joint fusion has an inherent loss of mobility, and patients may struggle on uneven ground. Risk of nonunion, deltoid insufficiency, and ankle valgus is also present.<ref name=":1" /> | ||
Stage IV disease management depends on whether there is a rigid flatfoot. Some patients progress to stage IV disease without rigid disease due to the failure of the deltoid ligament. In this setting, patients may have treatment with a deltoid ligament repair. Patients with rigid stage IV disease will require an ankle fusion, which is associated with significant morbidity. Ankle replacement is an alternative to arthrodesis.<ref name=":1" /><ref>Ketz J, Myerson M, Sanders R. The salvage of complex hindfoot problems with use of a custom talar total ankle prosthesis. J Bone Joint Surg Am. 2012 Jul 03;94(13):1194-200</ref> | |||
A recent meta-analysis of surgical treatments for adult acquired flatfoot was conducted to study the efficacy of different therapies further. This study analyzed different radiographic angles to measure the effectiveness of each procedure, including medial calcaneal osteotomies, lateral column lengthening, and double and triple arthrodesis. The conclusions of the study suggested that all treatment types result in significant improvements for the patient.<ref>Tao X, Chen W, Tang K. Surgical procedures for treatment of adult acquired flatfoot deformity: a network meta-analysis. J Orthop Surg Res. 2019 Feb 21;14(1):62</ref> | |||
== Prognosis == | == Prognosis == | ||
The prognosis for most patients with adult acquired flatfoot is favorable. Most patients will not need surgery. The approximately 10% that do require surgery can expect favorable outcomes. | The prognosis for most patients with adult acquired flatfoot is favorable. Most patients will not need surgery. The approximately 10% that do require surgery can expect favorable outcomes.<ref name=":6" /> The higher stage diseases require more extensive surgery, with stage IV adult acquired flatfoot requiring ankle fusion or total ankle arthroplasty.<ref name=":1" /> | ||
Adult acquired flatfoot that is left untreated can progress to more severe stages that require more invasive treatments. Early diagnosis is critical and can even help avoid surgery in some patients. As the disease progresses into late stages, the need for the patient to get an ankle fusion increases. With an ankle fusion, the patient essentially has an immobile ankle joint, and many recreational activities are affected. | Adult acquired flatfoot that is left untreated can progress to more severe stages that require more invasive treatments. Early diagnosis is critical and can even help avoid surgery in some patients. As the disease progresses into late stages, the need for the patient to get an ankle fusion increases. With an ankle fusion, the patient essentially has an immobile ankle joint, and many recreational activities are affected. | ||
== References == | == References == | ||
| Line 65: | Line 168: | ||
|license-link=https://creativecommons.org/licenses/by/4.0/ | |license-link=https://creativecommons.org/licenses/by/4.0/ | ||
}} | }} | ||
<references/> | |||
{{Reliable sources|synonym1=acquired flatfoot}} | |||
[[Category:Foot and Ankle Conditions]] | |||
[[Category:Foot and Ankle]] | |||
Revision as of 18:18, 10 November 2022

Adult acquired flatfoot (AAFD), formerly described as posterior tibial tendon dysfunction (PTTD) has complex pathology defined by the collapse of the medial longitudinal arch of the foot with continued progressive deformity of the foot and ankle. [1]
Anatomy
The anatomy of the foot and ankle are complex, with multiple structures involved in the stability and function needed to walk and bear weight.
A structure principally involved in the development of adult acquired flatfoot is the posterior tibialis tendon. In addition to plantar flexion, the posterior tibialis tendon is the primary inverter of the foot. It inserts principally on the navicular tuberosity, but also has lesser insertions on to other tarsal and metatarsal structures.[2]
The spring and deltoid ligaments are crucial to the stability of the foot and ankle. The spring ligament, which is the ligament most frequently involved in adult-acquired flatfoot, supports the ankle by connections from the sustentaculum tali of the calcaneus to the navicular. The primary role of the spring ligament is to support the head of the talus.[3] The deltoid ligament is usually affected later in the progression of the adult acquired flatfoot. The superficial deltoid ligament has a wide insertion on the navicular to the posterior tibiotalar capsule. It is the primary support against tibiotalar valgus angulation. The deep deltoid ligament prevents axial rotation of the talus, where it inserts, from its origin on the intercollicular groove and posterior colliculus. The deltoid ligament as a whole is critical in supporting the articulating surfaces of the ankle and the spring ligament.[4]
Development
All children are born with flat feet. Toddlers may walk with a flatfoot posture in order to have their feet resting entirely on the ground with their weight over the first or second tarsometatarsal joints. In most children the longitudinal arch develops by the time they are 10 years old. At this stage treatment is not indicated. However a full arch may not develop, and the persistence of physiological flexible flatfoot into adulthood is common.
Aetiology and Pathophysiology
Acquired flatfoot was historically attributed to posterior tibial tendon deficiency, although now the understanding is that the ligamentous structures of the ankle play a role in adult-acquired flatfoot development.[1][5] The dysfunction of the posterior tibial tendon is a multifactorial process. In many patients, there is a preexisting flatfoot, and many patients are also obese. Another factor is a relative hypovascularity of the tendon as it makes an abrupt turn posterior to the medial malleolus; this predisposes the tendon to rupture due to insufficient repair.[6] Episodes of previous trauma, corticosteroid injections, arthritis, neuromuscular conditions, and diabetes all predispose to the development of an adult acquired flatfoot.[7]
The posterior tibial tendon is critical in maintaining the appropriate gait and function of the foot. Contraction of the tibialis posterior causes inversion of the foot and locking of the transverse tarsal joints granting stability for push-off.[2] Deficiency of the posterior tibialis tendon leads to an unstable transverse tarsal joint and forefoot abduction, allowing unopposed action of the peroneus brevis. The ensuing abduction of the forefoot and transverse talar joints also displaces the force of the calcaneal tendon laterally, further accentuating the valgus defect of the foot.[8] The continued strain on the static stabilizing ligaments eventually leads to their attenuation. Most commonly, the spring ligament is affected, failure leads to medial and plantar subluxation of the talar head relative to the navicular. Failure of the deltoid ligament will lead to a valgus position of the talus within the ankle mortise.[1][2][4][9][7] These events may occur in a stepwise fashion, corresponding to Johnson and Strom classification system. However, some patients develop a valgus talar tilt without a fixed flatfoot deformity.[4]
Epidemiology
Acquired flatfoot is a common orthopaedic condition, although there is a relative paucity of literature on the epidemiology regarding adult acquired flatfoot. There are 5 million people in the United States affected with adult acquired flatfoot. In the UK, the estimated prevalence is estimated to be over 3% in women over 40 years old.[10] Posterior tibial tendon issues are prevalent in the geriatric population, with 10% of geriatric patients affected. The geriatric population might be predisposed to more severe adult acquired flatfoot due to the degeneration of muscle mass and bone structure, as well.[11] Patients with chronic vascular diseases are at increased risk; this includes diabetics and patients with hypertension.[7]
Classification
Acquired flatfoot grading is by the Johnson and Strom classification system, which has classification grades of I to III.[12] Myerson added a fourth grade in 1997.[13] The classification system aids practitioners in identifying AAFD severity and also can guide treatment plans.[5]
- Stage I: characteristically presents with posterior tibial tendon tenosynovitis with no arch collapse.
- Stage II: foot collapse and will be unable to perform a single-leg heel rise.
- Stage IIa: foot collapse with valgus deformity of the hindfoot but no midfoot abduction
- Stage IIb: midfoot abduction is present.
- Stage III: fixed deformity with hindfoot valgus and forefoot abduction.
- Stage IV: ankle valgus secondary to deltoid ligament attenuation.[9]
Assessment
It is essential to evaluate the patient with suspected adult acquired flatfoot during weight-bearing. There are specific hallmark findings of adult acquired flatfoot for which practitioners should look. While the patient is standing with the provider behind excessive abduction of the forefoot can be noted by the “too many toes” sign. This test is positive if the practitioner can see more than the fifth and part of the fourth toe. Inspection and palpation over the posterior tibial tendon at the area of the medial malleolus may demonstrate swelling or pain. On the lateral aspect of the foot pain may be elicited if there is impingement of ligamentous structures.[14] Single and double heel rise tests may be performed to assess the strength of the posterior tibial tendon. Failure to invert the foot on heel rise or perform heel rise at all is considered indicative of posterior tibial tendon dysfunction. Ankle range of motion requires assessment. Effort should be made to correct valgus deformity in a range of motion exercise to evaluate for fixed deformity. A fixed deformity of the subtalar joint or fixed abduction of the forefoot has implications in treatment.[2]
| Stage | Clinical Features | Pathology | Imaging |
|---|---|---|---|
| I |
|
|
|
| IIA |
|
|
|
| IIB |
|
|
|
| III |
|
|
|
| IV |
|
|
|
Differential Diagnosis
While the diagnosis of adult acquired flatfoot is relatively straightforward, the following differentials should be considered. A careful history and physical examination can usually rule out most of these conditions.[15]
- Flexible, Non-PTTD (physiological from childhood)
- Flexible, PTTD (flexible unless severe)
- Structural (tarsal coalition, accessory navicular)
- Inflammatory (RhA, Spondyloarthropathies)
- Degenerative
- Neurological (cerebral palsy)
- Post traumatic
Imaging
The gold standard for the evaluation of adult acquired flatfoot is weight-bearing radiographs. Radiographs are necessary in the anteroposterior, lateral, and hindfoot views. These views will assess the degree of arch collapse, particularly by measuring the lateral first tarsometatarsal angle, and forefoot abduction at the talonavicular joint. Talar head uncoverage can also be measured in the setting of stage IV disease by the lateral talonavicular angle. Lateral views of the foot can also display naviculocuneiform and first tarsometatarsal collapse. Arthritis should be carefully assessed on all radiographic films as this may have implications on treatment options.[14]
MRI is typically not needed for evaluation of adult acquired flatfoot; however, it may be beneficial for some patients with ligamentous involvement that may alter surgical treatment planning; this is particularly relevant for patients with medial peritalar instability, who have improved functional outcomes with deltoid-spring ligament reconstruction.[16]
Several studies indicate that ultrasound may be a useful modality in assessing the posterior tibial tendon when compared to the more time consuming and costly MRI. Results from an ultrasonographic evaluation of the posterior tibial tendon were equivalent to MRI in 87% to 94% of patients.[17][18]
Imaging Case
44 year old man with two year history of relapsing medial ankle pain. On exam has hindfoot valgus with medial arch collapse and tenderness over the medial column. Xray showed planovalgus foot with pes planus 20 degrees and hindfoot valgus 32 degrees. No significant radiographic osteoarthritis. Ultrasound showed the tibialis posterior tendon sheath to be very thickened with considerable adjacent vascularity. The tendon itself remained intact. Corticosteroid injection, orthotics, and a graded exercise programme were orgnaised.

AP xray

Lateral xray

Mortise xray

Weightberaing foot xray

Weightbearing foot xray
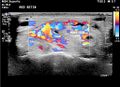
Tibialis posterior tenosynovitis






Management
The treatment of adult acquired flatfoot is complex. There are multiple treatment options, and the treatment of adult-acquired flatfoot has been the focus of most recent research. However, first-line therapy for the condition remains nonoperative.
Non-operative
Treatment with orthotic devices, such as low-articulating ankle-foot orthosis, cast-boot walkers, and other ankle-foot orthoses in conjunction with NSAID therapy and physical therapy have a resolution of symptoms 87% of the time according to one study. Other studies have success rates of 67 to 90% with conservative measures.[14]
Acquired flatfoot appears to be associated with obesity, diabetes, hypertension, and other disease processes that are treatable with a healthy lifestyle and weight reduction. Patients with adult acquired flatfoot may benefit from the treatment of their other medical comorbidities. Additionally, patients may prevent further disease progression once diagnosed with the use of an appropriate orthotic device. Most patients who use an orthotic device in conjunction with PT and or NSAID therapy will not need any surgical intervention.[14]
Surgery
Surgical treatment is indicated in patients who have attempted conservative therapy and are not satisfied with their results. Surgical treatment depends on the stage of the disease, as well as other factors including medical comorbidities, functional status, and use of tobacco.
Surgical management of stage I disease is uncommon, but if required patients should undergo posterior tibial tendon tenosynovectomy, debridement, or flexor digitorum longus tendon autograft. There is a concern that repair of the posterior tibial tendon may experience complications with long-term failure; therefore, surgical treatment should be carefully considered prior to any intervention.[9]
Stage II disease treatment has been successful by medializing calcaneal osteotomy in addition to a flexor digitorum longus transfer. One study showed 87% of patient satisfaction with this treatment after a mean follow-up of 15 years.[19]
Stage III disease becomes more challenging to treat due to the fixed nature of the defect. Arthrodesis is the standard of care, with double and triple arthrodesis being common. Double arthrodesis entails a fusion of the subtalar and talonavicular joints. Triple arthrodesis involves the calcaneocuboid joint in addition to the two joints mentioned above. Double arthrodesis has the advantage of reduced arthritic complications and reduced joint stiffness associated with calcaneocuboid fusion. Unfortunately, joint fusion has an inherent loss of mobility, and patients may struggle on uneven ground. Risk of nonunion, deltoid insufficiency, and ankle valgus is also present.[2]
Stage IV disease management depends on whether there is a rigid flatfoot. Some patients progress to stage IV disease without rigid disease due to the failure of the deltoid ligament. In this setting, patients may have treatment with a deltoid ligament repair. Patients with rigid stage IV disease will require an ankle fusion, which is associated with significant morbidity. Ankle replacement is an alternative to arthrodesis.[2][20]
A recent meta-analysis of surgical treatments for adult acquired flatfoot was conducted to study the efficacy of different therapies further. This study analyzed different radiographic angles to measure the effectiveness of each procedure, including medial calcaneal osteotomies, lateral column lengthening, and double and triple arthrodesis. The conclusions of the study suggested that all treatment types result in significant improvements for the patient.[21]
Prognosis
The prognosis for most patients with adult acquired flatfoot is favorable. Most patients will not need surgery. The approximately 10% that do require surgery can expect favorable outcomes.[14] The higher stage diseases require more extensive surgery, with stage IV adult acquired flatfoot requiring ankle fusion or total ankle arthroplasty.[2]
Adult acquired flatfoot that is left untreated can progress to more severe stages that require more invasive treatments. Early diagnosis is critical and can even help avoid surgery in some patients. As the disease progresses into late stages, the need for the patient to get an ankle fusion increases. With an ankle fusion, the patient essentially has an immobile ankle joint, and many recreational activities are affected.
References
Part or all of this article or section is derived from Adult Acquired Flatfoot by Abdul Arain; Michael C. Harrington; Andrew J. Rosenbaum., used under Creative Commons Attribution 4.0 International License
- ↑ 1.0 1.1 1.2 Deland JT. Adult-acquired flatfoot deformity. J Am Acad Orthop Surg. 2008 Jul;16(7):399-406. [PubMed]
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 Abousayed MM, Alley MC, Shakked R, Rosenbaum AJ. Adult-Acquired Flatfoot Deformity: Etiology, Diagnosis, and Management. JBJS Rev. 2017 Aug;5(8):e7.
- ↑ Bastias GF, Dalmau-Pastor M, Astudillo C, Pellegrini MJ. Spring Ligament Instability. Foot Ankle Clin. 2018 Dec;23(4):659-678.
- ↑ 4.0 4.1 4.2 Smith JT, Bluman EM. Update on stage IV acquired adult flatfoot disorder: when the deltoid ligament becomes dysfunctional. Foot Ankle Clin. 2012 Jun;17(2):351-60.
- ↑ 5.0 5.1 Abousayed MM, Tartaglione JP, Rosenbaum AJ, Dipreta JA. Classifications in Brief: Johnson and Strom Classification of Adult-acquired Flatfoot Deformity. Clin Orthop Relat Res. 2016 Feb;474(2):588-93.
- ↑ Petersen W, Hohmann G, Stein V, Tillmann B. The blood supply of the posterior tibial tendon. J Bone Joint Surg Br. 2002 Jan;84(1):141-4
- ↑ 7.0 7.1 7.2 Holmes GB, Mann RA. Possible epidemiological factors associated with rupture of the posterior tibial tendon. Foot Ankle. 1992 Feb;13(2):70-9
- ↑ Brodsky JW. Preliminary gait analysis results after posterior tibial tendon reconstruction: a prospective study. Foot Ankle Int. 2004 Feb;25(2):96-100
- ↑ 9.0 9.1 9.2 Smyth NA, Aiyer AA, Kaplan JR, Carmody CA, Kadakia AR. Adult-acquired flatfoot deformity. Eur J Orthop Surg Traumatol. 2017 May;27(4):433-439
- ↑ Kohls-Gatzoulis J, Woods B, Angel JC, Singh D. The prevalence of symptomatic posterior tibialis tendon dysfunction in women over the age of 40 in England. Foot Ankle Surg. 2009;15(2):75-81.
- ↑ Ikpeze TC, Brodell JD, Chen RE, Oh I. Evaluation and Treatment of Posterior Tibialis Tendon Insufficiency in the Elderly Patients. Geriatr Orthop Surg Rehabil. 2019;10:2151459318821461.
- ↑ Johnson KA, Strom DE. Tibialis posterior tendon dysfunction. Clin Orthop Relat Res. 1989 Feb;(239):196-206.
- ↑ Myerson MS. Adult acquired flatfoot deformity: treatment of dysfunction of the posterior tibial tendon. Instr Course Lect. 1997;46:393-405.
- ↑ 14.0 14.1 14.2 14.3 14.4 Vulcano E, Deland JT, Ellis SJ. Approach and treatment of the adult acquired flatfoot deformity. Curr Rev Musculoskelet Med. 2013 Dec;6(4):294-303
- ↑ Lee MS, Vanore JV, Thomas JL, Catanzariti AR, Kogler G, Kravitz SR, Miller SJ, Gassen SC., Clinical Practice Guideline Adult Flatfoot Panel. Diagnosis and treatment of adult flatfoot. J Foot Ankle Surg. 2005 Mar-Apr;44(2):78-113
- ↑ Brodell JD, MacDonald A, Perkins JA, Deland JT, Oh I. Deltoid-Spring Ligament Reconstruction in Adult Acquired Flatfoot Deformity With Medial Peritalar Instability. Foot Ankle Int. 2019 Jul;40(7):753-761.
- ↑ Arnoldner MA, Gruber M, Syré S, Kristen KH, Trnka HJ, Kainberger F, Bodner G. Imaging of posterior tibial tendon dysfunction--Comparison of high-resolution ultrasound and 3T MRI. Eur J Radiol. 2015 Sep;84(9):1777-81
- ↑ Harish S, Kumbhare D, O'Neill J, Popowich T. Comparison of sonography and magnetic resonance imaging for spring ligament abnormalities: preliminary study. J Ultrasound Med. 2008 Aug;27(8):1145-52
- ↑ Chadwick C, Whitehouse SL, Saxby TS. Long-term follow-up of flexor digitorum longus transfer and calcaneal osteotomy for stage II posterior tibial tendon dysfunction. Bone Joint J. 2015 Mar;97-B(3):346-52
- ↑ Ketz J, Myerson M, Sanders R. The salvage of complex hindfoot problems with use of a custom talar total ankle prosthesis. J Bone Joint Surg Am. 2012 Jul 03;94(13):1194-200
- ↑ Tao X, Chen W, Tang K. Surgical procedures for treatment of adult acquired flatfoot deformity: a network meta-analysis. J Orthop Surg Res. 2019 Feb 21;14(1):62
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,

