Ankle Joint Injection
| Ankle Joint Injection | |
|---|---|
| Indication | Ankle Osteoarthritis, and various rheumatological conditions |
| Syringe | 3mL |
| Needle | 22-25G 30mm |
| Steroid | 30mg triamcinolone |
| Local | 2-4mL lidocaine |
| Volume | 2-5mL |
Anatomy
- Main article: Ankle Joint Anatomy
The ankle joint, or tibiotalar joint, is a hinged synovial joint. It is created by the articulation of the distal end of the tibia, fibula, and the superior aspect of the talus. It provides dorsiflexion and plantarflexion. The classic mnemonic "Tom, Dick, and Harry" is used to remember the muscles that cross the anterior ankle joint in the medial plane - tibialis anterior, extensor hallucis longus, and extensor digitorum longus. These structures are held by the superior and inferior extensor retinacula. The lateral muscles are peroneus longus and brevis. These are supported by the superior and inferior peroneal retinaculum. The medial ligaments are the deltoid ligaments, and the lateral ligaments are the talofibular ligament (ATFL), calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL). The deep peroneal nerve and anterior tibial artery (anterior neurovascular bundle) cross the ankle joint between the extensor digitorum longus and extensor hallucis longus, and then descend into the dorsal aspect of the foot. The anterior tibial artery becomes the dorsalis pedis artery. The superficial peroneal nerve is found anterolaterally to the ankle joint.
Indications and Efficacy
Pain secondary to osteoarthritis, rheumatoid arthritis, acute traumatic arthritis, crystalloid deposition disease, mixed connective tissue disease, and synovitis.
Contraindications
Pre-procedural Evaluation
In the setting of significant joint space narrowing, the anteromedial approach may be difficult. The lateral approach may be more successful here.[1]
Equipment
- High frequency linear ultrasound probe
- 20 to 25 gauge 1.5 inch needle
- 1% lidocaine
- corticosteroid
- 5-mL syringe
- sterile ultrasound gel and cover
- dressing pack with sterile drape, gauze pad
- Sterile cleansing solution
- Adhesive bandage
Technique
Ultrasound Guided
- Patient supine, knee flexed about 90 degrees, with foot flat on the examination table in 30-45 degrees of plantar flexion
- Position the probe long-axis to the plantar flexed foot anteriorly just medial to the tibialis anterior tendon
- Confirm location of the anterior neurovascular bundle
- Localise the anterior recess of the tibiotalar joint
- Insert needle into the anteromedial joint space, long axis, distal to proximal at about a 30-degree angle, passing just over the talar dome, aiming towards the underside of the tibia.
- Position needle tip just past the joint capsule in the anterior recess of the joint

Probe position and needle placement. © Springer 2017
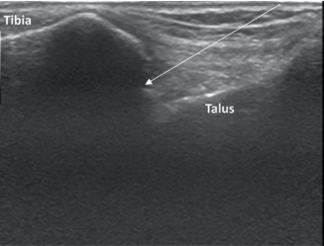
Ultrasound image


Fluoroscopy Guided
Landmark Guided

Medial Approach (tibiotalar)
- Position: Supine with foot perpendicular to leg
- Identify and mark sulcus, between the tibia and talus, lateral to the medial malleolus and medial to the tibialis anterior and extensor hallucis longus tendons
- Plantarflex the foot with needle entering the skin overlying the sulcus
- Angle the needle slightly cranially as it passes between the medial malleolus and tibialis anterior tendon
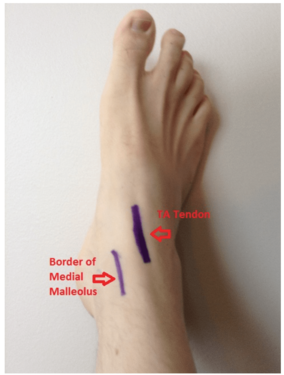
Medial approach: enter space between anterior border of the medial malleolus and the tibialis anterior tendon

Medial approach: have patient lie supine, and plantar flex the ankle so the angle is close to 90 degrees.


Lateral Approach (subtalar)
- Keep foot perpendicular to leg
- Enter subtalar joint just below tip of lateral malleolus
- Direct needle medially toward joint space
Complications
Injury to the neurovascular bundle.
Aftercare
Videos
See Also
External Links
References
- ↑ Manchikanti, Laxmaiah, et al. Essentials of interventional techniques in managing chronic pain. Cham: Springer, 2018.
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,

