Gluteal Tendinopathy: Difference between revisions
No edit summary |
|||
| (31 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
{{ | {{Authors | ||
Greater trochanteric pain syndrome (GTPS) | |Authors=EmilyG | ||
==Aetiology and Pathophysiology == | |Additional contributors=Jeremy | ||
Gluteal tendinopathy is caused by | |Peer reviewer=Jeremy | ||
|Review complete=Yes | |||
}} | |||
{{Condition | |||
|quality=Peer reviewed | |||
|image=Greater trochanter facets.png | |||
|caption=The four facets of a right greater trochanter. The [[Gluteus Medius|gluteus medius]] inserts at the superoposterior and lateral facets; [[Gluteus Minimus|gluteus minimus]] inserts at the anterior facet. | |||
|epidemiology=Women aged over 40 | |||
|pathophysiology=Overload [[Tendinopathy|degenerative tendinopathy]] of [[Gluteus Medius|gluteus medius]] and/or [[Gluteus Minimus|gluteus minimus]] tendons. | |||
|clinicalfeatures=Chronic lateral hip pain that is exacerbated by activity and side-lying. Greater trochanteric tenderness and pain provocation in tests assessing the use of the hip abductors. | |||
|diagnosis=Clinical diagnosis with no accepted criteria | |||
|tests=Usually not required but can include X-ray, Ultrasound, MRI. | |||
|ddx=[[Hip Osteoarthritis|Hip osteoarthritis]], Lumbar spine [[Somatic Referred Pain|somatic referred pain]]. | |||
|treatment=Load management, avoidance of compressive forces, graded exercise programme, injections, surgery. | |||
|prognosis=Usually self-limiting | |||
}} | |||
'''Gluteal tendinopathy''', referring to tendinopathy of gluteus medius and/or gluteus minimus tendons, is the most common cause of lateral hip pain and can lead to severe disability. Load management and graded strengthening is primary treatment. | |||
==Terminology== | |||
Greater trochanteric pain syndrome (GTPS) is an umbrella term encompassing different musculoskeletal entities that may contribute to chronic lateral hip pain including gluteus medius and minimus tendinopathy/ tears, trochanteric bursitis, and [[Snapping Hip Syndrome|external coxa saltans]]. | |||
Any bursal distension (sub-gluteal minimus/medius) is invariably secondary to or co-exists with an underlying gluteal tendinopathy. The tendinopathy is a non-inflammatory condition. Therefore the term "trochanteric bursitis" (and the related terms "trochanteritis") is generally regarded as a misnomer.<ref name=":7">{{Cite journal|last=Grimaldi|first=Alison|last2=Mellor|first2=Rebecca|last3=Hodges|first3=Paul|last4=Bennell|first4=Kim|last5=Wajswelner|first5=Henry|last6=Vicenzino|first6=Bill|date=2015-08|title=Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management|url=http://link.springer.com/10.1007/s40279-015-0336-5|journal=Sports Medicine|language=en|volume=45|issue=8|pages=1107–1119|doi=10.1007/s40279-015-0336-5|issn=0112-1642}}</ref> Primary trochanteric bursitis is very rare, and microbiological causes should be considered in those cases. | |||
==Anatomy== | |||
The peri-trochanteric space is the interval located between the greater trochanter and the [[Gluteus Maximus|gluteus maximus]], [[Tensor Fascia Lata|tensor fascia lata]], and iliotibial band. The peri-trochanteric space contains the hip abductors: [[Gluteus Medius|gluteus medius]], [[Gluteus Minimus|gluteus minimus]], and [[Tensor Fascia Lata|tensor fascia lata]]. | |||
In the "rotator cuff of the hip" there are six external rotators, three internal rotators, two trochanteric abductors, and three iliotibial band tensioners. | |||
*The external rotators are [[piriformis]], [[Gemelli Muscles|gemellus superior and inferior]], [[Obturator Internus|obturator internus]], [[Obturator Externus|obturator externus]], and [[Quadratus Femoris|quadratus femoris]]. | |||
*The internal rotators are [[Gluteus Minimus|gluteus minimus]], [[Gluteus Medius|gluteus medius]], and [[Tensor Fascia Lata|tensor fascia lata]] | |||
*The trochanteric abductors are [[Gluteus Minimus|gluteus minimus]] and [[Gluteus Medius|gluteus medius]]. | |||
*The iliotibial band tensioners are [[Tensor Fascia Lata|tensor fascia lata]], [[Gluteus Maximus|gluteus maximus]], and [[Vastus Lateralis|vastus lateralis]]. | |||
The greater trochanter has four facets (anterior, lateral, posterior, and superoposteiror) with three tendon insertions. | |||
[[Gluteus Medius|Gluteus medius]] is the most important muscle in gluteal tendinopathy. It is a large fan-shaped muscle that has its origin at the outer edge of the iliac crest running from the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS). It has three equal portions: anterior, middle, and posterior. The anterior and middle portions with its vertically oriented muscle fibres assist with initiating hip abduction. The posterior portion with its horizontally oriented fibres is active in heel strike to full stance during gait to stabilise the hip. It inserts at the superoposterior and lateral facets of the greater trochanter. | |||
[[Gluteus Minimus|Gluteus minimus]] has its orrigin from the gluteal surface of the ilium. It inserts onto the lateral facet and onto the hip capsule on the anterior facet, called the long head and capsular head respectively. There is a "bald spot" between the capsular attachment and the lateral facet. | |||
There are three bursa in the lateral hip. The subgluteus medius bursa overlies the superior part of the lateral facet. The gluteus minimus bursa lies over the lateral facet. The subgluteus maximus mursa lies between the [[Gluteus Maximus|gluteus maximus]] and iliotibial band. | |||
<gallery widths="300" heights="300"> | |||
File:Posterior Hip Muscles 2.png|gluteus medius shown on the right | |||
File:Posterior_Hip_Muscles.png|gluteus minimus shown on the right | |||
File:Lateral hip illustration and cadaver.jpg|lateral hip with foot prints of gluteus medius, gluteus minimus, and vastus lateralis | |||
File:Greater trochanter anatomy facets insertions and bursae.jpg|Anatomy of the greater trochanter. (a) Three peritrochanteric bursae, (b) osseous facets of the greater trochanter, and (c) insertion sites for the abductor tendons<ref>{{Cite journal|last=Pianka|first=Mark A.|last2=Serino|first2=Joseph|last3=DeFroda|first3=Steven F.|last4=Bodendorfer|first4=Blake M.|date=2021|title=Greater trochanteric pain syndrome: Evaluation and management of a wide spectrum of pathology|url=https://pubmed.ncbi.nlm.nih.gov/34158938|journal=SAGE open medicine|volume=9|pages=20503121211022582|doi=10.1177/20503121211022582|issn=2050-3121|pmc=8182177|pmid=34158938}}</ref> | |||
</gallery> | |||
==Aetiology and Pathophysiology== | |||
{{See also|Tendinopathy}} | |||
Historically lateral hip pain was thought to be exclusively due to trochanteric bursitis. However it is now understood that tendon tears are the source of pain, and the presence of any bursitis is merely an epiphenomenon. | |||
A healthy tendon has a homeostatic balance between anabolic and catabolic processes. Gluteal tendinopathy is caused by disturbance in this balance following a combination of excessive compression and high tensile loads. The tendon is particularly susceptible when there is a rapid increase in intensity of load without giving the tendon time to adapt.<ref name=":1">{{Cite journal|last=Grimaldi|first=Alison|last2=Mellor|first2=Rebecca|last3=Hodges|first3=Paul|last4=Bennell|first4=Kim|last5=Wajswelner|first5=Henry|last6=Vicenzino|first6=Bill|date=2015-05-13|title=Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management|url=http://dx.doi.org/10.1007/s40279-015-0336-5|journal=Sports Medicine|volume=45|issue=8|pages=1107–1119|doi=10.1007/s40279-015-0336-5|issn=0112-1642}}</ref><ref name=":2">{{Cite journal|last=Cook|first=J L|last2=Purdam|first2=C R|date=2008-09-23|title=Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy|url=http://dx.doi.org/10.1136/bjsm.2008.051193|journal=British Journal of Sports Medicine|volume=43|issue=6|pages=409–416|doi=10.1136/bjsm.2008.051193|issn=0306-3674}}</ref> This could be due to a traumatic event (e.g. direct blow) or a frequent and repeated exposure to a load (e.g. jumping athlete).<ref name=":2" /><ref name=":1" /> | |||
Three continuous stages of disease have been described: normal to reactive tendinopathy to tendon dysrepair to degenerative tendinopathy.<ref name=":1" /> Tendon tears can be intrasubstance, partial, or complete. This is explained in more detail in [[Tendinopathy]]. It is difficult to manage because pain is not closely connected to progression of pathology.<ref name=":2" /> | |||
==Epidemiology and Risk Factors== | ==Epidemiology and Risk Factors== | ||
Gluteal tendinopathy is a common condition with a prevalence that is highest in women in their fourth to sixth decades.<ref name=":1" /> One study reporting 23.5% of females and 8.5% of men between 50-79 years being affected in community-based population.<ref>{{Cite journal|last=Segal|first=Neil A.|last2=Torner|first2=James|last3=Xie|first3=Hui|last4=Felson|first4=David|last5=Curtis|first5=Jeffrey R.|last6=Nevitt|first6=Michael|date=2006-11-01|title=PR_092: Greater Trochanteric Pain Syndrome: Epidemiology and Associated Factors|url=https://www.archives-pmr.org/article/S0003-9993(06)01018-5/fulltext|journal=Archives of Physical Medicine and Rehabilitation|language=English|volume=87|issue=11|pages=e20|doi=10.1016/j.apmr.2006.08.114|issn=0003-9993}}</ref> A rapid increase in intensity and/or frequency of loads on gluteal tendons puts individuals at risk.<ref name=":2" /> Both athletes and sedentary individuals are affected.<ref name=":1" /> Higher body weight is another association.<ref>{{Cite journal|last=Plinsinga|first=Melanie Louise|last2=Ross|first2=Megan Heather|last3=Coombes|first3=Brooke Kaye|last4=Vicenzino|first4=Bill|date=2019-10|title=Physical findings differ between individuals with greater trochanteric pain syndrome and healthy controls: A systematic review with meta-analysis|url=https://linkinghub.elsevier.com/retrieve/pii/S2468781219300074|journal=Musculoskeletal Science and Practice|language=en|volume=43|pages=83–90|doi=10.1016/j.msksp.2019.07.009}}</ref> | |||
==Clinical Features== | ==Clinical Features== | ||
=== History=== | ===History=== | ||
The patient typically complains of dull aching pain over the lateral hip. The onset is typically slow but can occur following a traumatic event (fall, forceful sporting action). The pain is typically worsened with time and can be associated with a change in physical activity. Pain can [[Somatic Referred Pain|radiate]] to the buttock and/or down the lateral thigh. Associated symptom of stiffness of hip on standing or walking following sitting. Sleep can be significantly disturbed as pain is typically worse at night time and pain makes it difficult to sleep on the side.<ref name=":1" /> | |||
Pain can cause significant disability, particularly with single leg standing activities e.g. dressing, walking and going up stairs or hills.<ref name=":1" /> Patients with gluteal tendinopathy have levels of disability that is comparable to patients with severe [[Hip Osteoarthritis|hip osteoarthritis]].<ref>{{Cite journal|last=Bohn|first=Marie Bagger|last2=Lund|first2=Bent|last3=Spoorendonk|first3=Kasper|last4=Lange|first4=Jeppe|date=2021-05-28|title=Gluteal-related lateral hip pain|url=https://pubmed.ncbi.nlm.nih.gov/34704929|journal=Danish Medical Journal|volume=68|issue=6|pages=A01210027|issn=2245-1919|pmid=34704929}}</ref> | |||
===Examination=== | ===Examination=== | ||
'''Gait:''' The patient is assessed during [[gait]] to evaluate for a Trendelenburg pattern. This test is highly specific but not sensitive, and is more suggestive of advanced disease.<ref name=":6" /> | |||
'''Tenderness to palpation of the greater trochanter:''' This is a considered a cardinal sign. Any absence of tenderness should raise suspicion for an alternative diagnosis.<ref name=":7" /> | |||
'''Sustained single-leg stance (Trendelenburg Test)''': Lateral hip pain reproduced on 30s single-leg stance test has a sensitivity and specificity of 100% and 97.3% respectively for gluteal tendinopathy. The high utility of the test is only maintained if the patient is instructed not to hitch the pelvis into relative abduction (where there is reduced tendon compression load). The examiner may provide gentle fingertip support to steady the patient.<ref name=":1" /> | |||
'''Resisted abduction test''': performed with the patient in lateral decubitus. It has a 73% sensitivity and 87% specificity. Patients with decreased hip power are more likely to fail non operative management.<ref name=":6" /> | |||
'''Resisted internal rotation test:''' See figure for picture and instructions. It is more accurate than Trendelenburg gait, greater trochanteric tenderness, and resisted abduction. This test is based on the function of gluteus medius as an internal rotator, with the internal rotation torque increased in a position of hip flexion. It has a sensitivity of 92% and specificity of 85% for the detection of gluteus medius tears. Note, this is different to the external derotation test which has the patient at significantly greater external rotation which is less specific to the hip abductors.<ref name=":6" /> | |||
'''FABER:''' The FABER test is useful in the differential diagnosis as limited range of movement is associated with hip joint pathology but not gluteal tendinopathy.<ref name=":1" /> | |||
The lumbosacral spine should also be examined. | |||
'''Leg Length Measurement:''' Gross [[Leg Length Discrepancy|leg length discrepancy]] may contribute to GTPS. The examiner stands behind the patient, paces their hands over the iliac crests, and estimates if they are level. Another method is measuring from the ASIS to the tip of the medial malleolus.<ref>{{Cite journal|last=Campbell|first=T. Mark|last2=Ghaedi|first2=Bahareh Bahram|last3=Tanjong Ghogomu|first3=Elizabeth|last4=Welch|first4=Vivian|date=2018-05|title=Shoe Lifts for Leg Length Discrepancy in Adults With Common Painful Musculoskeletal Conditions: A Systematic Review of the Literature|url=https://pubmed.ncbi.nlm.nih.gov/29229292|journal=Archives of Physical Medicine and Rehabilitation|volume=99|issue=5|pages=981–993.e2|doi=10.1016/j.apmr.2017.10.027|issn=1532-821X|pmid=29229292}}</ref> | |||
'''Ober's test:''' has been shown to lack diagnostic utility for gluteal tendinopathy.<ref name=":1" /> | |||
<gallery widths="300" heights="300"> | |||
File:Gluteus medius tear resisted internal rotation test.jpg|The resisted internal rotation test. Patient is supine with affected hip and knee at 90° flexion and hip at 10° external rotation. The patient actively internally rotates the hip against resistance (knee away and foot towards examiner in photo). The test is positive with pain reproduction or weakness.<ref name=":6">{{Cite journal|last=Ortiz-Declet|first=Victor|last2=Chen|first2=Austin W|last3=Maldonado|first3=David R|last4=Yuen|first4=Leslie C|last5=Mu|first5=Brian|last6=Domb|first6=Benjamin G|date=2019-12-01|title=Diagnostic accuracy of a new clinical test (resisted internal rotation) for detection of gluteus medius tears|url=https://academic.oup.com/jhps/article/6/4/398/5625718|journal=Journal of Hip Preservation Surgery|language=en|volume=6|issue=4|pages=398–405|doi=10.1093/jhps/hnz046|issn=2054-8397|pmc=PMC6990389|pmid=32015892}}</ref> | |||
File:Hip abductor strength testing.jpg|Resisted abduction test. Pain or weakness with resisted abduction in lateral decubitus with the affected side up. | |||
File:Trendelenburg test.jpg|Trendelenburg test. The test is positive if the contralateral pelvis tilts downwards when asked to stand on the affected foot. | |||
</gallery> | |||
==Investigations== | ==Investigations== | ||
MRI and | [[File:Gluteus medius MRI high grade partial thickness tear.jpg|thumb|450x450px|(a) Coronal fat suppressed proton density and (b) sagittal T2-weighted sequences on MRI of the right hip showing a high-grade partial tear of the gluteus medius and minimus tendons with tendinosis and underlying trochanteric bursitis.<ref>{{Cite journal|last=Pianka|first=Mark A|last2=Serino|first2=Joseph|last3=DeFroda|first3=Steven F|last4=Bodendorfer|first4=Blake M|date=2021-01|title=Greater trochanteric pain syndrome: Evaluation and management of a wide spectrum of pathology|url=http://journals.sagepub.com/doi/10.1177/20503121211022582|journal=SAGE Open Medicine|language=en|volume=9|pages=205031212110225|doi=10.1177/20503121211022582|issn=2050-3121|pmc=PMC8182177|pmid=34158938}}</ref>]] | ||
MRI is gold standard as it can visualise changes associated with gluteal tendinopathy, such as tendon thickening and soft tissue oedema, the clearest.<ref name=":1" /> MRI is also useful in excluding other causes of lateral hip pain.<ref name=":1" /> However, MRI is expensive and not very accessible.<ref name=":1" /> Consequently, ultrasound is typically used in clinical practice.<ref name=":1" /> The accuracy of ultrasound in identifying gluteal tendinopathy is variable and dependent on operator experience and patient characteristics.<ref name=":1" /> It is important to note that it is normal for radiological changes to be present in the asymptomatic population, thus, any findings need to be considered within the clinical context.<ref name=":1" /> | |||
===Imaging Findings=== | ===Imaging Findings=== | ||
<u>Xray</u> | |||
Plain radiographs are helpful for ruling out [[Hip Osteoarthritis|hip osteoarthritis]], [[Femoroacetabular Impingement|femoroacetabular impingement]], and [[Calcific Tendinopathy|calcific tendinopathy]]. However pincer-type FAI may be associated with the development of GTPS.<ref name=":8">{{Cite journal|last=Sunil Kumar|first=Karadi Hari|last2=Rawal|first2=Jaikirty|last3=Nakano|first3=Naoki|last4=Sarmento|first4=André|last5=Khanduja|first5=Vikas|date=2021-08|title=Pathogenesis and contemporary diagnoses for lateral hip pain: a scoping review|url=https://link.springer.com/10.1007/s00167-020-06354-1|journal=Knee Surgery, Sports Traumatology, Arthroscopy|language=en|volume=29|issue=8|pages=2408–2416|doi=10.1007/s00167-020-06354-1|issn=0942-2056}}</ref> | |||
<u>Ultrasound</u> | |||
Ultrasound is operator dependent. It has a higher PPV than MRI when done by an experienced musculoskeletal radiologist.<ref name=":8" /> Findings include:<ref name=":3">{{Cite journal|last=Kong|first=Andrew|last2=Van der Vliet|first2=Andrew|last3=Zadow|first3=Steven|date=2006-12-06|title=MRI and US of gluteal tendinopathy in greater trochanteric pain syndrome|url=http://dx.doi.org/10.1007/s00330-006-0485-x|journal=European Radiology|volume=17|issue=7|pages=1772–1783|doi=10.1007/s00330-006-0485-x|issn=0938-7994}}</ref> | |||
*Thickened tendons | |||
*Reduced echogenicity of tendons | |||
*More heterogeneous echogenicity of tendons | |||
*Increased echogenicity of muscles as reduced muscle bulk and increased fat | |||
*Partial tears are indicated by thinning of the tendon and partial thickness area free from echo | |||
*Complete tears are indicated by the full thickness of the tender being free from echo and a “bald” facet | |||
*Deep to gluteus tendon insertions there may be cortical irregularities | |||
On Doppler Ultrasound uncommonly one can see increased vascularity<ref name=":3" /> | |||
<u>MRI</u><ref>{{Cite journal|last=Dadour|first=Joseph Rudy|last2=Gilbert|first2=Guillaume|last3=Lepage-Saucier|first3=Marianne|last4=Freire|first4=Véronique|last5=Bureau|first5=Nathalie J.|date=2021-04-29|title=Quantitative MRI in patients with gluteal tendinopathy and asymptomatic volunteers: initial results on T1- and T2*-mapping diagnostic accuracy and correlation with clinical assessment|url=http://dx.doi.org/10.1007/s00256-021-03781-0|journal=Skeletal Radiology|volume=50|issue=11|pages=2221–2231|doi=10.1007/s00256-021-03781-0|issn=0364-2348}}</ref> | |||
Tears on MRI are classified as tendinosis, partial-thickness, or full-thickness. Findings do not correlate well with symptoms, with abnormalities seen in 50% of patients without lateral hip pain.<ref>{{Cite journal|last=Blankenbaker|first=Donna G.|last2=Ullrick|first2=Steven R.|last3=Davis|first3=Kirkland W.|last4=De Smet|first4=Arthur A.|last5=Haaland|first5=Ben|last6=Fine|first6=Jason P.|date=2008-10|title=Correlation of MRI findings with clinical findings of trochanteric pain syndrome|url=https://pubmed.ncbi.nlm.nih.gov/18566811|journal=Skeletal Radiology|volume=37|issue=10|pages=903–909|doi=10.1007/s00256-008-0514-8|issn=0364-2348|pmid=18566811}}</ref> | |||
*Tendinosis is suggested by hyperintensity in T2-weighted images within the tendon of gluteus minimus and/or gluteus medius | |||
*Fluid distension of the greater trochanteric bursa | |||
*On coronal T1-weighted imaging there may be fatty streaks or fatty infiltration of gluteus minimus and/or gluteus medius | |||
*Partial tears are indicated by hyperintensity in T2 view within the tendon of gluteus minimus and/or gluteus medius along with a thickened tendon. | |||
*Partial tears can presents with or without tendon thinning | |||
*Complete tears are indicated by disruption of the tendon of gluteus minimus and/or gluteus medius | |||
*Osseous avulsion may or may not be present in a complete tear | |||
===Other Investigations=== | ===Other Investigations=== | ||
Other imaging techniques are currently being developed. These include ultrasound tissue characterisation and elastography.<ref name=":1" /> | |||
==Diagnosis== | ==Diagnosis== | ||
No clear diagnostic criteria exists for gluteal tendinopathy.<ref name=":4">{{Cite journal|last=Reid|first=Diane|date=2016-03|title=The management of greater trochanteric pain syndrome: A systematic literature review|url=http://dx.doi.org/10.1016/j.jor.2015.12.006|journal=Journal of Orthopaedics|volume=13|issue=1|pages=15–28|doi=10.1016/j.jor.2015.12.006|issn=0972-978X}}</ref> Typically the diagnosis is made clinically.<ref name=":4" /> The history most commonly involves lateral hip pain that is exacerbated by activity and lying on the affected side.<ref name=":4" /> On examination, one would expect to find tenderness on palpation of the greater trochanter.<ref name=":4" /> This is the most common clinical finding in gluteal tendinopathy.<ref name=":4" /> | |||
[[Hip Osteoarthritis|Hip osteoarthritis]] is a common differential diagnosis for lateral hip pain. Asking about difficulty in manipulating shoes and socks is a useful way to differentiate the conditions.<ref name=":5">{{Cite journal|last=Fearon|first=Angela M|last2=Scarvell|first2=Jennie M|last3=Neeman|first3=Terry|last4=Cook|first4=Jill L|last5=Cormick|first5=Wes|last6=Smith|first6=Paul N|date=2013-07|title=Greater trochanteric pain syndrome: defining the clinical syndrome|url=https://bjsm.bmj.com/lookup/doi/10.1136/bjsports-2012-091565|journal=British Journal of Sports Medicine|language=en|volume=47|issue=10|pages=649–653|doi=10.1136/bjsports-2012-091565|issn=0306-3674}}</ref> A paper published in the British Journal of Sports Medicine suggested that diagnostic criteria for gluteal tendinopathy should include the patient reporting to have no difficulty in manipulating socks and shoes.<ref name=":5" /> This paper also suggested the diagnostic criteria to include lateral hip pain reproduced on the FABER test as the FABER test should not produce lateral hip pain in hip osteoarthritis.<ref name=":5" /> | |||
==Differential Diagnosis== | ==Differential Diagnosis== | ||
{{DDX Box|ddx-title=Differential Diagnosis of Lateral Hip Pain|ddx-text={{Lateral Hip Pain DDX}}}} | |||
==Treatment== | ==Treatment== | ||
Gluteal tendinopathy for the majority is self limiting. It has been reported that more than 90% of people are responsive to conservative treatment. Those who are not are considered refractory cases.<ref name=":4" /> Conservative treatment can include patient education, physiotherapy, [[Nonsteroidal Anti-Inflammatory Drugs|NSAIDs]], corticosteroid injections (CSI), shockwave therapy, and PRP injections. There are varying levels of evidence for each of these interventions. Evidence does not support the conservative treatment of deep transverse friction massage, therapeutic ultrasound and acupuncture.<ref name=":4" /> | |||
===Education=== | |||
Patients should be advised to avoid sitting with crossed legs, sit with hips higher than knees, stand evenly on both feet and hip width apart, avoid lying on the painful hip and place a pillow under the top leg if side-lying, sleep on the back if possible, continue exercising as tolerated, but avoid aggravating exercise.<ref name=":9">{{Cite journal|last=Mellor|first=Rebecca|last2=Bennell|first2=Kim|last3=Grimaldi|first3=Alison|last4=Nicolson|first4=Philippa|last5=Kasza|first5=Jessica|last6=Hodges|first6=Paul|last7=Wajswelner|first7=Henry|last8=Vicenzino|first8=Bill|date=2018-05-02|title=Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial|url=http://dx.doi.org/10.1136/bmj.k1662|journal=BMJ|pages=k1662|doi=10.1136/bmj.k1662|issn=0959-8138}}</ref> | |||
===Exercise=== | |||
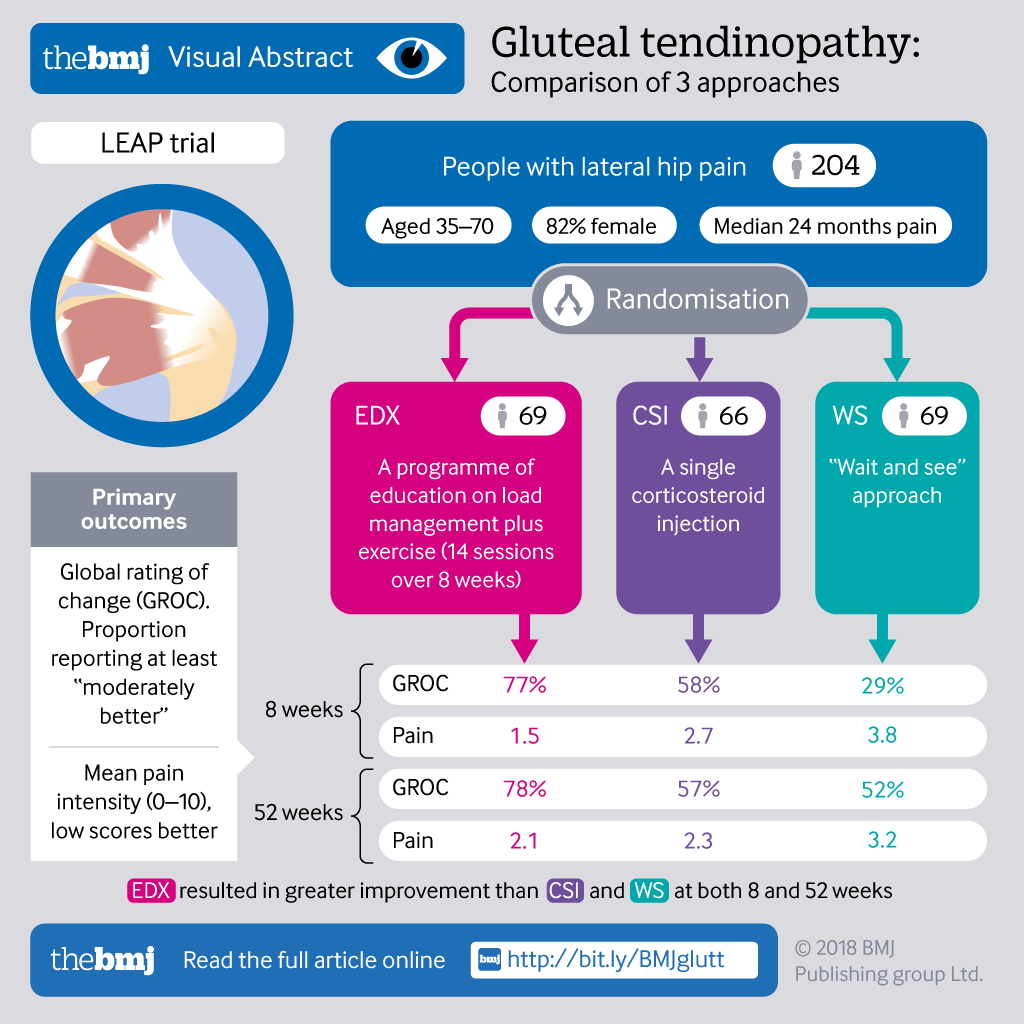
Physiotherapy that is based around graded exercise has been shown to be effective in other tendinopathies. There is no universally recommended treatment protocol for gluteal tendinopathy.<ref name=":4" /> The LEAP protocol has shown promise when compared to no treatment and a single corticosteroid injection. The LEAP protocol involves education on load management (e.g. avoiding lying on side of affected leg) and a specific graded exercise programme.<ref name=":9" /> This study and its results can be found in the resources below and the [[Media:Gluteal tendinopathy va v12.png|infographic]]. | |||
The | The concept of an activity ladder can be used. The patient should state an activity goal. Start at low tendon load such as swimming with gentle kicking or other water based activities. Progress through medium pace walking or bicycling on the flat, to bicycling with a gradual slope, to faster paced walking or bicycling, to slow running intervals on the flat, to walking up hills and stairs, to running and a medium to high pace, to running up and down hills, finally to plyometrics. The patient stops progressing at their desired goal. Pain can be used as a guide to know if the load is manageable for the tendon, with low levels of pain meaning that the load is not excessive. | ||
=== | ===Injections=== | ||
There is some evidence for injection therapies.<ref>{{Cite journal|last=Ladurner|first=Andreas|last2=Fitzpatrick|first2=Jane|last3=O’Donnell|first3=John M.|date=2021-07-01|title=Treatment of Gluteal Tendinopathy: A Systematic Review and Stage-Adjusted Treatment Recommendation|url=http://journals.sagepub.com/doi/10.1177/23259671211016850|journal=Orthopaedic Journal of Sports Medicine|language=en|volume=9|issue=7|pages=232596712110168|doi=10.1177/23259671211016850|issn=2325-9671|pmc=PMC8330465|pmid=34377713}}</ref> Common injectates are corticosteroid and leukocyte rich [[Platelet Rich Plasma Injection|platelet rich plasma]] (LR-PRP). The injectate is deposited around the tendon or sometimes into the tendon itself. Ultrasound can be used for needle guidance, however no significant difference between ultrasound guided and blind injection outcomes have been found.<ref name=":4" /> corticosteroid may provide benefit in the short term but with a high recurrence rate and poorer results in the long term. | |||
=== | Given the paucity of treatments for chronic gluteal tendinopathy (>3 months) and transient amelioration effect of CSI, there is interest whether biologic products such as PRP may provide better long-term outcomes for this condition.<ref name=":0">{{Cite journal|last=Koulischer|first=Simon|last2=Callewier|first2=Antoine|last3=Zorman|first3=David|date=June 2017|title=Management of greater trochanteric pain syndrome : a systematic review|url=https://pubmed.ncbi.nlm.nih.gov/30399983|journal=Acta Orthopaedica Belgica|volume=83|issue=2|pages=205–214|doi=|issn=0001-6462|pmid=30399983|via=|doi-access=}}</ref> The use of PRP has been controversial. Technician skills, method of preparation, patient variables, and the grade of tendinopathy used can all potentially alter effectiveness. | ||
=== Surgery === | ===Surgery=== | ||
Gluteal tendon reconstruction is experimental with no standardised techniques.<ref name=":0" /> | Gluteal tendon reconstruction is experimental with no standardised techniques.<ref name=":0" /> If surgery is done it involves a combination of some of the following procedures: bursectomy, ITB release, trochanteric reduction osteotomy and gluteal tendon repair.<ref name=":4" /> | ||
==Follow Up and Prognosis== | ==Follow Up and Prognosis== | ||
Over 90% respond to conservative treatment but there are still large number of patients thar fail non-operative treatment with significant levels of dysfunction making it important to find novel treatment strategies. | |||
==Summary== | ==Summary== | ||
== | *Aetiology and pathophysiology for gluteal tendinopathy remains incompletely known. | ||
*Prevalence is highest in women over 40 years | |||
*Both athletes and sedentary individuals are affected | |||
*History of lateral hip pain | |||
*Examination of lateral hip pain reproduced on FABER test and 30s single-leg stance test | |||
*No set diagnostic criteria | |||
*Diagnosis is typically clinical | |||
*Imaging can be done with MRI being gold standard but ultrasound more clinically available | |||
*No universally prescribed treatment protocol but LEAP protocol provides some promise | |||
*Conservative treatment effective in more than 90% of cases | |||
==Resources== | |||
{{PDF|Grimaldi2015_-_Gluteal_Tendinopathy.pdf|Gluteal Tendinopathy - Grimaldi 2015|caption=Good review article from a physiotherapy perspective}} | {{PDF|Grimaldi2015_-_Gluteal_Tendinopathy.pdf|Gluteal Tendinopathy - Grimaldi 2015|caption=Good review article from a physiotherapy perspective}} | ||
{{PDF|Pathogenesis and contemporary diagnoses for lateral hip pain - Kumar 2020.pdf|Pathogenesis and contemporary diagnoses for lateral hip pain - Kumar 2020|caption=Review on the causes of lateral hip pain}} | |||
{{PDF|Greater trochanteric pain syndrome simplified MRI approach - Amin 2022.pdf|Greater trochanteric pain syndrome simplified MRI approach - Amin 2022}} | |||
{{PDF|Mellor2018_-_Leap_Trial.pdf|LEAP Trial - Mellor 2018|caption=Important RCT comparing corticosteroid to structured load management}} | {{PDF|Mellor2018_-_Leap_Trial.pdf|LEAP Trial - Mellor 2018|caption=Important RCT comparing corticosteroid to structured load management}} | ||
{{PDF|LEAP_Protocol.pdf|LEAP Protocol}} | {{PDF|LEAP_Protocol.pdf|LEAP Protocol}} | ||
== Links == | ==External Links== | ||
[https://dralisongrimaldi.com/blog/how-physiotherapists-treat-gluteal-tendinopathy/ How physiotherapists treat gluteal tendinopathy by Dr Alison Grimaldi] | [https://dralisongrimaldi.com/blog/how-physiotherapists-treat-gluteal-tendinopathy/ How physiotherapists treat gluteal tendinopathy by Dr Alison Grimaldi] | ||
==References== | ==References== | ||
[[Category:Pelvis, Hip and Thigh Conditions]] | |||
[[Category: | |||
[[Category:Tendinopathies]] | [[Category:Tendinopathies]] | ||
<references /> | |||
{{References}} | |||
{{Reliable sources | |||
|synonym1=Trochanteric+Bursitis | |||
|synonym2=Greater+Trochanteric+Pain+Syndrome | |||
}} | |||
Latest revision as of 16:24, 23 April 2022

| |
| Gluteal Tendinopathy | |
|---|---|
| Epidemiology | Women aged over 40 |
| Pathophysiology | Overload degenerative tendinopathy of gluteus medius and/or gluteus minimus tendons. |
| Clinical Features | Chronic lateral hip pain that is exacerbated by activity and side-lying. Greater trochanteric tenderness and pain provocation in tests assessing the use of the hip abductors. |
| Diagnosis | Clinical diagnosis with no accepted criteria |
| Tests | Usually not required but can include X-ray, Ultrasound, MRI. |
| DDX | Hip osteoarthritis, Lumbar spine somatic referred pain. |
| Treatment | Load management, avoidance of compressive forces, graded exercise programme, injections, surgery. |
| Prognosis | Usually self-limiting |
Gluteal tendinopathy, referring to tendinopathy of gluteus medius and/or gluteus minimus tendons, is the most common cause of lateral hip pain and can lead to severe disability. Load management and graded strengthening is primary treatment.
Terminology
Greater trochanteric pain syndrome (GTPS) is an umbrella term encompassing different musculoskeletal entities that may contribute to chronic lateral hip pain including gluteus medius and minimus tendinopathy/ tears, trochanteric bursitis, and external coxa saltans.
Any bursal distension (sub-gluteal minimus/medius) is invariably secondary to or co-exists with an underlying gluteal tendinopathy. The tendinopathy is a non-inflammatory condition. Therefore the term "trochanteric bursitis" (and the related terms "trochanteritis") is generally regarded as a misnomer.[1] Primary trochanteric bursitis is very rare, and microbiological causes should be considered in those cases.
Anatomy
The peri-trochanteric space is the interval located between the greater trochanter and the gluteus maximus, tensor fascia lata, and iliotibial band. The peri-trochanteric space contains the hip abductors: gluteus medius, gluteus minimus, and tensor fascia lata.
In the "rotator cuff of the hip" there are six external rotators, three internal rotators, two trochanteric abductors, and three iliotibial band tensioners.
- The external rotators are piriformis, gemellus superior and inferior, obturator internus, obturator externus, and quadratus femoris.
- The internal rotators are gluteus minimus, gluteus medius, and tensor fascia lata
- The trochanteric abductors are gluteus minimus and gluteus medius.
- The iliotibial band tensioners are tensor fascia lata, gluteus maximus, and vastus lateralis.
The greater trochanter has four facets (anterior, lateral, posterior, and superoposteiror) with three tendon insertions.
Gluteus medius is the most important muscle in gluteal tendinopathy. It is a large fan-shaped muscle that has its origin at the outer edge of the iliac crest running from the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS). It has three equal portions: anterior, middle, and posterior. The anterior and middle portions with its vertically oriented muscle fibres assist with initiating hip abduction. The posterior portion with its horizontally oriented fibres is active in heel strike to full stance during gait to stabilise the hip. It inserts at the superoposterior and lateral facets of the greater trochanter.
Gluteus minimus has its orrigin from the gluteal surface of the ilium. It inserts onto the lateral facet and onto the hip capsule on the anterior facet, called the long head and capsular head respectively. There is a "bald spot" between the capsular attachment and the lateral facet.
There are three bursa in the lateral hip. The subgluteus medius bursa overlies the superior part of the lateral facet. The gluteus minimus bursa lies over the lateral facet. The subgluteus maximus mursa lies between the gluteus maximus and iliotibial band.
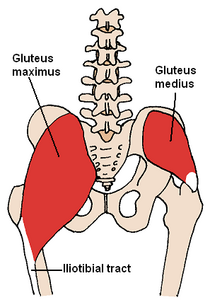
gluteus medius shown on the right
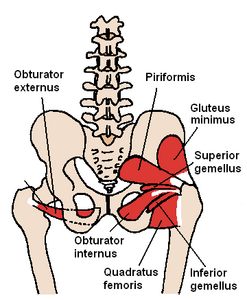
gluteus minimus shown on the right
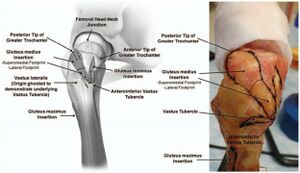
lateral hip with foot prints of gluteus medius, gluteus minimus, and vastus lateralis
![Anatomy of the greater trochanter. (a) Three peritrochanteric bursae, (b) osseous facets of the greater trochanter, and (c) insertion sites for the abductor tendons[2]](/w/img_auth.php/thumb/4/4c/Greater_trochanter_anatomy_facets_insertions_and_bursae.jpg/300px-Greater_trochanter_anatomy_facets_insertions_and_bursae.jpg)
Anatomy of the greater trochanter. (a) Three peritrochanteric bursae, (b) osseous facets of the greater trochanter, and (c) insertion sites for the abductor tendons[2]



![Anatomy of the greater trochanter. (a) Three peritrochanteric bursae, (b) osseous facets of the greater trochanter, and (c) insertion sites for the abductor tendons[2]](/wiki/File:Greater_trochanter_anatomy_facets_insertions_and_bursae.jpg)
Aetiology and Pathophysiology
- See also: Tendinopathy
Historically lateral hip pain was thought to be exclusively due to trochanteric bursitis. However it is now understood that tendon tears are the source of pain, and the presence of any bursitis is merely an epiphenomenon.
A healthy tendon has a homeostatic balance between anabolic and catabolic processes. Gluteal tendinopathy is caused by disturbance in this balance following a combination of excessive compression and high tensile loads. The tendon is particularly susceptible when there is a rapid increase in intensity of load without giving the tendon time to adapt.[3][4] This could be due to a traumatic event (e.g. direct blow) or a frequent and repeated exposure to a load (e.g. jumping athlete).[4][3]
Three continuous stages of disease have been described: normal to reactive tendinopathy to tendon dysrepair to degenerative tendinopathy.[3] Tendon tears can be intrasubstance, partial, or complete. This is explained in more detail in Tendinopathy. It is difficult to manage because pain is not closely connected to progression of pathology.[4]
Epidemiology and Risk Factors
Gluteal tendinopathy is a common condition with a prevalence that is highest in women in their fourth to sixth decades.[3] One study reporting 23.5% of females and 8.5% of men between 50-79 years being affected in community-based population.[5] A rapid increase in intensity and/or frequency of loads on gluteal tendons puts individuals at risk.[4] Both athletes and sedentary individuals are affected.[3] Higher body weight is another association.[6]
Clinical Features
History
The patient typically complains of dull aching pain over the lateral hip. The onset is typically slow but can occur following a traumatic event (fall, forceful sporting action). The pain is typically worsened with time and can be associated with a change in physical activity. Pain can radiate to the buttock and/or down the lateral thigh. Associated symptom of stiffness of hip on standing or walking following sitting. Sleep can be significantly disturbed as pain is typically worse at night time and pain makes it difficult to sleep on the side.[3]
Pain can cause significant disability, particularly with single leg standing activities e.g. dressing, walking and going up stairs or hills.[3] Patients with gluteal tendinopathy have levels of disability that is comparable to patients with severe hip osteoarthritis.[7]
Examination
Gait: The patient is assessed during gait to evaluate for a Trendelenburg pattern. This test is highly specific but not sensitive, and is more suggestive of advanced disease.[8]
Tenderness to palpation of the greater trochanter: This is a considered a cardinal sign. Any absence of tenderness should raise suspicion for an alternative diagnosis.[1]
Sustained single-leg stance (Trendelenburg Test): Lateral hip pain reproduced on 30s single-leg stance test has a sensitivity and specificity of 100% and 97.3% respectively for gluteal tendinopathy. The high utility of the test is only maintained if the patient is instructed not to hitch the pelvis into relative abduction (where there is reduced tendon compression load). The examiner may provide gentle fingertip support to steady the patient.[3]
Resisted abduction test: performed with the patient in lateral decubitus. It has a 73% sensitivity and 87% specificity. Patients with decreased hip power are more likely to fail non operative management.[8]
Resisted internal rotation test: See figure for picture and instructions. It is more accurate than Trendelenburg gait, greater trochanteric tenderness, and resisted abduction. This test is based on the function of gluteus medius as an internal rotator, with the internal rotation torque increased in a position of hip flexion. It has a sensitivity of 92% and specificity of 85% for the detection of gluteus medius tears. Note, this is different to the external derotation test which has the patient at significantly greater external rotation which is less specific to the hip abductors.[8]
FABER: The FABER test is useful in the differential diagnosis as limited range of movement is associated with hip joint pathology but not gluteal tendinopathy.[3]
The lumbosacral spine should also be examined.
Leg Length Measurement: Gross leg length discrepancy may contribute to GTPS. The examiner stands behind the patient, paces their hands over the iliac crests, and estimates if they are level. Another method is measuring from the ASIS to the tip of the medial malleolus.[9]
Ober's test: has been shown to lack diagnostic utility for gluteal tendinopathy.[3]
![The resisted internal rotation test. Patient is supine with affected hip and knee at 90° flexion and hip at 10° external rotation. The patient actively internally rotates the hip against resistance (knee away and foot towards examiner in photo). The test is positive with pain reproduction or weakness.[8]](/w/img_auth.php/thumb/8/80/Gluteus_medius_tear_resisted_internal_rotation_test.jpg/300px-Gluteus_medius_tear_resisted_internal_rotation_test.jpg)
The resisted internal rotation test. Patient is supine with affected hip and knee at 90° flexion and hip at 10° external rotation. The patient actively internally rotates the hip against resistance (knee away and foot towards examiner in photo). The test is positive with pain reproduction or weakness.[8]

Resisted abduction test. Pain or weakness with resisted abduction in lateral decubitus with the affected side up.

Trendelenburg test. The test is positive if the contralateral pelvis tilts downwards when asked to stand on the affected foot.
![The resisted internal rotation test. Patient is supine with affected hip and knee at 90° flexion and hip at 10° external rotation. The patient actively internally rotates the hip against resistance (knee away and foot towards examiner in photo). The test is positive with pain reproduction or weakness.[8]](/wiki/File:Gluteus_medius_tear_resisted_internal_rotation_test.jpg)


Investigations

MRI is gold standard as it can visualise changes associated with gluteal tendinopathy, such as tendon thickening and soft tissue oedema, the clearest.[3] MRI is also useful in excluding other causes of lateral hip pain.[3] However, MRI is expensive and not very accessible.[3] Consequently, ultrasound is typically used in clinical practice.[3] The accuracy of ultrasound in identifying gluteal tendinopathy is variable and dependent on operator experience and patient characteristics.[3] It is important to note that it is normal for radiological changes to be present in the asymptomatic population, thus, any findings need to be considered within the clinical context.[3]
Imaging Findings
Xray
Plain radiographs are helpful for ruling out hip osteoarthritis, femoroacetabular impingement, and calcific tendinopathy. However pincer-type FAI may be associated with the development of GTPS.[11]
Ultrasound
Ultrasound is operator dependent. It has a higher PPV than MRI when done by an experienced musculoskeletal radiologist.[11] Findings include:[12]
- Thickened tendons
- Reduced echogenicity of tendons
- More heterogeneous echogenicity of tendons
- Increased echogenicity of muscles as reduced muscle bulk and increased fat
- Partial tears are indicated by thinning of the tendon and partial thickness area free from echo
- Complete tears are indicated by the full thickness of the tender being free from echo and a “bald” facet
- Deep to gluteus tendon insertions there may be cortical irregularities
On Doppler Ultrasound uncommonly one can see increased vascularity[12]
MRI[13]
Tears on MRI are classified as tendinosis, partial-thickness, or full-thickness. Findings do not correlate well with symptoms, with abnormalities seen in 50% of patients without lateral hip pain.[14]
- Tendinosis is suggested by hyperintensity in T2-weighted images within the tendon of gluteus minimus and/or gluteus medius
- Fluid distension of the greater trochanteric bursa
- On coronal T1-weighted imaging there may be fatty streaks or fatty infiltration of gluteus minimus and/or gluteus medius
- Partial tears are indicated by hyperintensity in T2 view within the tendon of gluteus minimus and/or gluteus medius along with a thickened tendon.
- Partial tears can presents with or without tendon thinning
- Complete tears are indicated by disruption of the tendon of gluteus minimus and/or gluteus medius
- Osseous avulsion may or may not be present in a complete tear
Other Investigations
Other imaging techniques are currently being developed. These include ultrasound tissue characterisation and elastography.[3]
Diagnosis
No clear diagnostic criteria exists for gluteal tendinopathy.[15] Typically the diagnosis is made clinically.[15] The history most commonly involves lateral hip pain that is exacerbated by activity and lying on the affected side.[15] On examination, one would expect to find tenderness on palpation of the greater trochanter.[15] This is the most common clinical finding in gluteal tendinopathy.[15]
Hip osteoarthritis is a common differential diagnosis for lateral hip pain. Asking about difficulty in manipulating shoes and socks is a useful way to differentiate the conditions.[16] A paper published in the British Journal of Sports Medicine suggested that diagnostic criteria for gluteal tendinopathy should include the patient reporting to have no difficulty in manipulating socks and shoes.[16] This paper also suggested the diagnostic criteria to include lateral hip pain reproduced on the FABER test as the FABER test should not produce lateral hip pain in hip osteoarthritis.[16]
Differential Diagnosis
- Gluteal Tendinopathy
- Hip (femoroacetabular) osteoarthrosis
- Somatic Referred Pain from the Lumbar Spine or Sacroiliac Joints
- Calcific Tendinopathy of the abductor tendons
- Meralgia paresthetica
- Snapping hip syndrome
- Femoroacetabular Impingement
- Proximal iliotibial band syndrome
- Apophysitis of the pelvis and hip
- Acetabular labral pathology
- Lumbar Spinal Stenosis
- Lumbar Radicular Pain
- Piriformis syndrome
- Morel-Lavallée lesion
- Post-traumatic haematoma, seroma, or lymphocele.
- Soft tissue tumour
- Femoral head avascular necrosis
- Femoral neck fracture
- Femoral neck stress fracture
- Iliopsoas tendinopathy
- Sports hernia
- Fibromyalgia
- Myofascial trigger points
- Complex regional pain syndrome
- Referred pain from intra-abdominal processes
Treatment
Gluteal tendinopathy for the majority is self limiting. It has been reported that more than 90% of people are responsive to conservative treatment. Those who are not are considered refractory cases.[15] Conservative treatment can include patient education, physiotherapy, NSAIDs, corticosteroid injections (CSI), shockwave therapy, and PRP injections. There are varying levels of evidence for each of these interventions. Evidence does not support the conservative treatment of deep transverse friction massage, therapeutic ultrasound and acupuncture.[15]
Education
Patients should be advised to avoid sitting with crossed legs, sit with hips higher than knees, stand evenly on both feet and hip width apart, avoid lying on the painful hip and place a pillow under the top leg if side-lying, sleep on the back if possible, continue exercising as tolerated, but avoid aggravating exercise.[17]
Exercise
Physiotherapy that is based around graded exercise has been shown to be effective in other tendinopathies. There is no universally recommended treatment protocol for gluteal tendinopathy.[15] The LEAP protocol has shown promise when compared to no treatment and a single corticosteroid injection. The LEAP protocol involves education on load management (e.g. avoiding lying on side of affected leg) and a specific graded exercise programme.[17] This study and its results can be found in the resources below and the infographic.
The concept of an activity ladder can be used. The patient should state an activity goal. Start at low tendon load such as swimming with gentle kicking or other water based activities. Progress through medium pace walking or bicycling on the flat, to bicycling with a gradual slope, to faster paced walking or bicycling, to slow running intervals on the flat, to walking up hills and stairs, to running and a medium to high pace, to running up and down hills, finally to plyometrics. The patient stops progressing at their desired goal. Pain can be used as a guide to know if the load is manageable for the tendon, with low levels of pain meaning that the load is not excessive.
Injections
There is some evidence for injection therapies.[18] Common injectates are corticosteroid and leukocyte rich platelet rich plasma (LR-PRP). The injectate is deposited around the tendon or sometimes into the tendon itself. Ultrasound can be used for needle guidance, however no significant difference between ultrasound guided and blind injection outcomes have been found.[15] corticosteroid may provide benefit in the short term but with a high recurrence rate and poorer results in the long term.
Given the paucity of treatments for chronic gluteal tendinopathy (>3 months) and transient amelioration effect of CSI, there is interest whether biologic products such as PRP may provide better long-term outcomes for this condition.[19] The use of PRP has been controversial. Technician skills, method of preparation, patient variables, and the grade of tendinopathy used can all potentially alter effectiveness.
Surgery
Gluteal tendon reconstruction is experimental with no standardised techniques.[19] If surgery is done it involves a combination of some of the following procedures: bursectomy, ITB release, trochanteric reduction osteotomy and gluteal tendon repair.[15]
Follow Up and Prognosis
Over 90% respond to conservative treatment but there are still large number of patients thar fail non-operative treatment with significant levels of dysfunction making it important to find novel treatment strategies.
Summary
- Aetiology and pathophysiology for gluteal tendinopathy remains incompletely known.
- Prevalence is highest in women over 40 years
- Both athletes and sedentary individuals are affected
- History of lateral hip pain
- Examination of lateral hip pain reproduced on FABER test and 30s single-leg stance test
- No set diagnostic criteria
- Diagnosis is typically clinical
- Imaging can be done with MRI being gold standard but ultrasound more clinically available
- No universally prescribed treatment protocol but LEAP protocol provides some promise
- Conservative treatment effective in more than 90% of cases
Resources
External Links
How physiotherapists treat gluteal tendinopathy by Dr Alison Grimaldi
References
- ↑ 1.0 1.1 Grimaldi, Alison; Mellor, Rebecca; Hodges, Paul; Bennell, Kim; Wajswelner, Henry; Vicenzino, Bill (2015-08). "Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management". Sports Medicine (in English). 45 (8): 1107–1119. doi:10.1007/s40279-015-0336-5. ISSN 0112-1642. Check date values in:
|date=(help) - ↑ Pianka, Mark A.; Serino, Joseph; DeFroda, Steven F.; Bodendorfer, Blake M. (2021). "Greater trochanteric pain syndrome: Evaluation and management of a wide spectrum of pathology". SAGE open medicine. 9: 20503121211022582. doi:10.1177/20503121211022582. ISSN 2050-3121. PMC 8182177. PMID 34158938.
- ↑ 3.00 3.01 3.02 3.03 3.04 3.05 3.06 3.07 3.08 3.09 3.10 3.11 3.12 3.13 3.14 3.15 3.16 Grimaldi, Alison; Mellor, Rebecca; Hodges, Paul; Bennell, Kim; Wajswelner, Henry; Vicenzino, Bill (2015-05-13). "Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management". Sports Medicine. 45 (8): 1107–1119. doi:10.1007/s40279-015-0336-5. ISSN 0112-1642.
- ↑ 4.0 4.1 4.2 4.3 Cook, J L; Purdam, C R (2008-09-23). "Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy". British Journal of Sports Medicine. 43 (6): 409–416. doi:10.1136/bjsm.2008.051193. ISSN 0306-3674.
- ↑ Segal, Neil A.; Torner, James; Xie, Hui; Felson, David; Curtis, Jeffrey R.; Nevitt, Michael (2006-11-01). "PR_092: Greater Trochanteric Pain Syndrome: Epidemiology and Associated Factors". Archives of Physical Medicine and Rehabilitation (in English). 87 (11): e20. doi:10.1016/j.apmr.2006.08.114. ISSN 0003-9993.
- ↑ Plinsinga, Melanie Louise; Ross, Megan Heather; Coombes, Brooke Kaye; Vicenzino, Bill (2019-10). "Physical findings differ between individuals with greater trochanteric pain syndrome and healthy controls: A systematic review with meta-analysis". Musculoskeletal Science and Practice (in English). 43: 83–90. doi:10.1016/j.msksp.2019.07.009. Check date values in:
|date=(help) - ↑ Bohn, Marie Bagger; Lund, Bent; Spoorendonk, Kasper; Lange, Jeppe (2021-05-28). "Gluteal-related lateral hip pain". Danish Medical Journal. 68 (6): A01210027. ISSN 2245-1919. PMID 34704929.
- ↑ 8.0 8.1 8.2 8.3 Ortiz-Declet, Victor; Chen, Austin W; Maldonado, David R; Yuen, Leslie C; Mu, Brian; Domb, Benjamin G (2019-12-01). "Diagnostic accuracy of a new clinical test (resisted internal rotation) for detection of gluteus medius tears". Journal of Hip Preservation Surgery (in English). 6 (4): 398–405. doi:10.1093/jhps/hnz046. ISSN 2054-8397. PMC 6990389. PMID 32015892.CS1 maint: PMC format (link)
- ↑ Campbell, T. Mark; Ghaedi, Bahareh Bahram; Tanjong Ghogomu, Elizabeth; Welch, Vivian (2018-05). "Shoe Lifts for Leg Length Discrepancy in Adults With Common Painful Musculoskeletal Conditions: A Systematic Review of the Literature". Archives of Physical Medicine and Rehabilitation. 99 (5): 981–993.e2. doi:10.1016/j.apmr.2017.10.027. ISSN 1532-821X. PMID 29229292. Check date values in:
|date=(help) - ↑ Pianka, Mark A; Serino, Joseph; DeFroda, Steven F; Bodendorfer, Blake M (2021-01). "Greater trochanteric pain syndrome: Evaluation and management of a wide spectrum of pathology". SAGE Open Medicine (in English). 9: 205031212110225. doi:10.1177/20503121211022582. ISSN 2050-3121. PMC 8182177. PMID 34158938. Check date values in:
|date=(help)CS1 maint: PMC format (link) - ↑ 11.0 11.1 Sunil Kumar, Karadi Hari; Rawal, Jaikirty; Nakano, Naoki; Sarmento, André; Khanduja, Vikas (2021-08). "Pathogenesis and contemporary diagnoses for lateral hip pain: a scoping review". Knee Surgery, Sports Traumatology, Arthroscopy (in English). 29 (8): 2408–2416. doi:10.1007/s00167-020-06354-1. ISSN 0942-2056. Check date values in:
|date=(help) - ↑ 12.0 12.1 Kong, Andrew; Van der Vliet, Andrew; Zadow, Steven (2006-12-06). "MRI and US of gluteal tendinopathy in greater trochanteric pain syndrome". European Radiology. 17 (7): 1772–1783. doi:10.1007/s00330-006-0485-x. ISSN 0938-7994.
- ↑ Dadour, Joseph Rudy; Gilbert, Guillaume; Lepage-Saucier, Marianne; Freire, Véronique; Bureau, Nathalie J. (2021-04-29). "Quantitative MRI in patients with gluteal tendinopathy and asymptomatic volunteers: initial results on T1- and T2*-mapping diagnostic accuracy and correlation with clinical assessment". Skeletal Radiology. 50 (11): 2221–2231. doi:10.1007/s00256-021-03781-0. ISSN 0364-2348.
- ↑ Blankenbaker, Donna G.; Ullrick, Steven R.; Davis, Kirkland W.; De Smet, Arthur A.; Haaland, Ben; Fine, Jason P. (2008-10). "Correlation of MRI findings with clinical findings of trochanteric pain syndrome". Skeletal Radiology. 37 (10): 903–909. doi:10.1007/s00256-008-0514-8. ISSN 0364-2348. PMID 18566811. Check date values in:
|date=(help) - ↑ 15.0 15.1 15.2 15.3 15.4 15.5 15.6 15.7 15.8 15.9 Reid, Diane (2016-03). "The management of greater trochanteric pain syndrome: A systematic literature review". Journal of Orthopaedics. 13 (1): 15–28. doi:10.1016/j.jor.2015.12.006. ISSN 0972-978X. Check date values in:
|date=(help) - ↑ 16.0 16.1 16.2 Fearon, Angela M; Scarvell, Jennie M; Neeman, Terry; Cook, Jill L; Cormick, Wes; Smith, Paul N (2013-07). "Greater trochanteric pain syndrome: defining the clinical syndrome". British Journal of Sports Medicine (in English). 47 (10): 649–653. doi:10.1136/bjsports-2012-091565. ISSN 0306-3674. Check date values in:
|date=(help) - ↑ 17.0 17.1 Mellor, Rebecca; Bennell, Kim; Grimaldi, Alison; Nicolson, Philippa; Kasza, Jessica; Hodges, Paul; Wajswelner, Henry; Vicenzino, Bill (2018-05-02). "Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial". BMJ: k1662. doi:10.1136/bmj.k1662. ISSN 0959-8138.
- ↑ Ladurner, Andreas; Fitzpatrick, Jane; O’Donnell, John M. (2021-07-01). "Treatment of Gluteal Tendinopathy: A Systematic Review and Stage-Adjusted Treatment Recommendation". Orthopaedic Journal of Sports Medicine (in English). 9 (7): 232596712110168. doi:10.1177/23259671211016850. ISSN 2325-9671. PMC 8330465. PMID 34377713.CS1 maint: PMC format (link)
- ↑ 19.0 19.1 Koulischer, Simon; Callewier, Antoine; Zorman, David (June 2017). "Management of greater trochanteric pain syndrome : a systematic review". Acta Orthopaedica Belgica. 83 (2): 205–214. ISSN 0001-6462. PMID 30399983.
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,


{kind=link}