Gluteal Tendinopathy
Greater trochanteric pain syndrome (GTPS) constitute a large number of musculoskeletal related presentations at the physician’s office. GTPS is an umbrella term encompassing different clinical entities that may contribute to chronic intermittent lateral hip pain. Multiple labels such as “trochanteric bursitis” and “tronchanteritis” have been used in the past which is now regarded as a misnomer. Invariably, the inflamed or enlarged bursa due to friction (sub-gluteal minimus/medius) is secondary or co-exist with an underlying pathology. Gluteal tendinopathy is identified as one of the major culprits of GTPS along with iliotibial band (ITB) and tensor fascia lata (TFT) as potential causes.
Epidemiolology
Gluteal tendinopathy has a propensity for middle-aged women, between 40 and 60 years.
Clinical Features
Pain tends to be localized to the bony greater trochanter with aggravating activities such as walking, stair climbing and lying on the affected side.
Investigations
MRIand ultrasound are useful Imaging tools to evaluate abnormalities of the lateral hip.
Treatment
Acute cases (<3 months) tend to be responsive to conservative measures such as physiotherapy, strengthening exercises, acupuncture, shock-wave therapy, corticosteroid injections and NSAIDs.[1]
Injections
Ultrasound can be used for needle guidance. The injectate is deposited directly on the bone and around the injections or into the tendon itself.
CSI may provide benefit in the short term but with a high recurrence rate and poorer results in the long term. Given the paucity of treatments for chronic gluteal tendinopathy (>3 months) and transient amelioration effect of CSI, there is interest whether biologic products such as PRP may provide better long-term outcomes for this condition[2]
The use of PRP has been controversial, especially in tendinopathies given its slower onset of action to see its efficacy. Some tendons respond differently to PRP. Technician skills, type on condition being treated and type of PRP used are all variables that can affect its effectiveness.
Activity Modification
Avoid compression.
Exercise
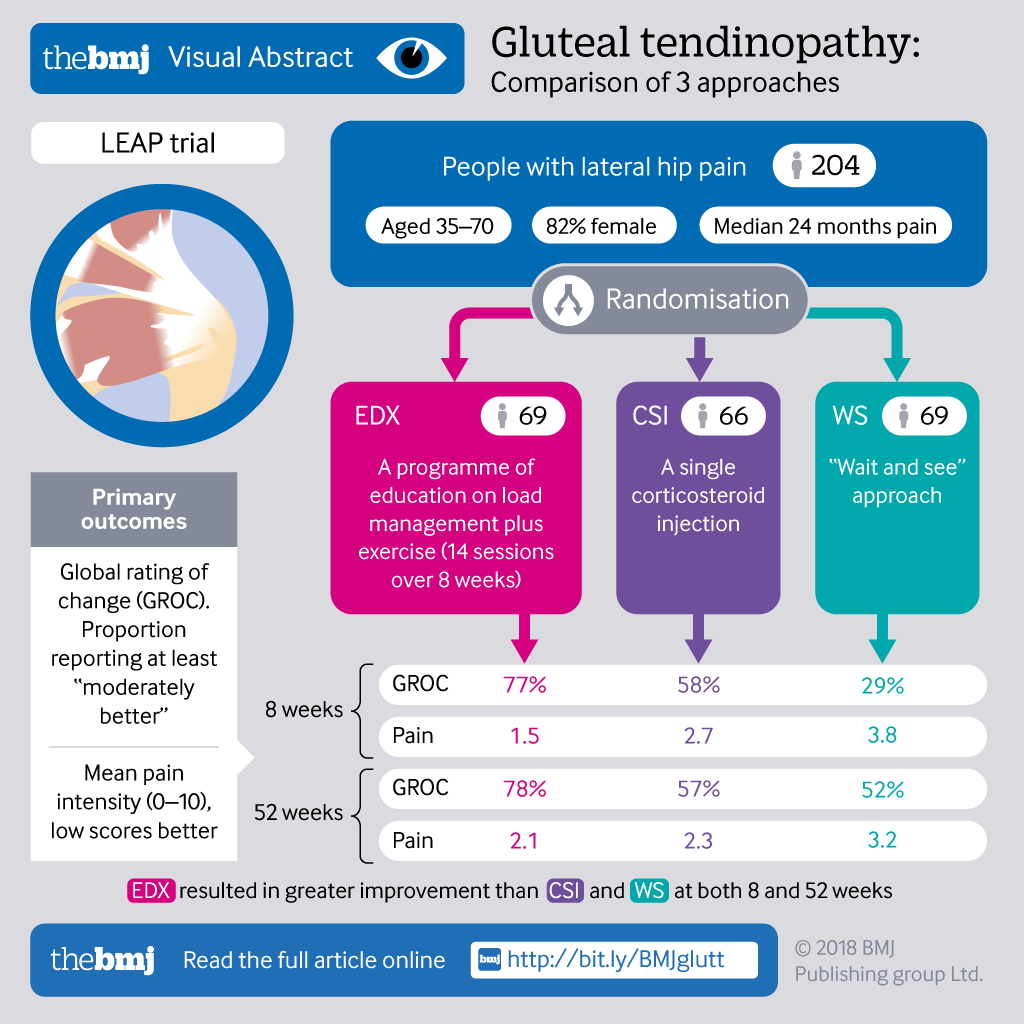
Leap Trial
Surgery
Gluteal tendon reconstruction is experimental with no standardised techniques.[1]
Prognosis
Large number of patients fail non-operative treatment with significant levels of dysfunction making important to find novel treatment strategies.
Downloads
Links
How physiotherapists treat gluteal tendinopathy by Dr Alison Grimaldi
References
- ↑ 1.0 1.1 Koulischer, Simon; Callewier, Antoine; Zorman, David (June 2017). Acta Orthopaedica Belgica. 83 (2): 205–214. ISSN 0001-6462. PMID 30399983 https://pubmed.ncbi.nlm.nih.gov/30399983. Text "Management of greater trochanteric pain syndrome : a systematic review" ignored (help); Missing or empty
|title=(help) - ↑ Fitzpatrick, Jane; Bulsara, Max K.; O’Donnell, John; Zheng, Ming Hao (April 2019). The American Journal of Sports Medicine (in English). 47 (5): 1130–1137. doi:10.1177/0363546519826969. ISSN 0363-5465 http://journals.sagepub.com/doi/10.1177/0363546519826969. Text "Leucocyte-Rich Platelet-Rich Plasma Treatment of Gluteus Medius and Minimus Tendinopathy: A Double-Blind Randomized Controlled Trial With 2-Year Follow-up" ignored (help); Missing or empty
|title=(help)
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,


{kind=link}