Gluteal Tendinopathy
Greater trochanteric pain syndrome (GTPS) constitute a large number of musculoskeletal related presentations at the physician’s office. GTPS is an umbrella term encompassing different clinical entities that may contribute to chronic intermittent lateral hip pain. Multiple labels such as “trochanteric bursitis” and “tronchanteritis” have been used in the past which is now regarded as a misnomer. Invariably, the inflamed or enlarged bursa due to friction (sub-gluteal minimus/medius) is secondary or co-exist with an underlying pathology. Gluteal tendinopathy is identified as one of the major culprits of GTPS along with iliotibial band (ITB) and tensor fascia lata (TFT) as potential causes.
Aetiology and Pathophysiology
Gluteal tendinopathy is caused by exposure to load that the tendon did not have adequate adaption or recovery time in order manage.[1][2] This could be due to a traumatic event (e.g. direct blow) or a frequent and repeated exposure to a load (e.g. jumping athlete).[2][1] Three continuous stages of disease have been described: normal to reactive tendinopathy to tendon dysrepair to degenerative tendinopathy.[1] This is explained in more detail in Tendinopathy. It is difficult because pain is not closely connected to progression of pathology.[2]
Epidemiology and Risk Factors
Common condition with prevalence highest in women over 40 years old.[1] One study reporting 23.5% of females and 8.5% of men between 50-79 years being affected in community-based population.[3] A rapid increase in intensity and/or frequency of on gluteal tendons puts individuals at risk.[2] Both athletes and sedentary individuals are affected.[1]
Clinical Features
History
Lateral hip pain over greater trochanter.[1] Onset typically slow but can occur following a traumatic event (fall, forceful sporting action).[1] Pain typically worsened with time and can be associated with a change in physical activity.[1] Pain can radiate around the trochanter and down the lateral thigh.[1] Associated symptom of stiffness of hip on standing or walking following sitting.[1] Sleep can be significantly disturbed as pain is typically worse at night time and pain makes it difficult for sleeping on side.[1] Pain can cause significant disability, particularly with single leg standing activities e.g. dressing, walking and going up stairs or hills.[1]
Examination
The most important sign is pain on palpation of the greater trochanter.[1] Absence of pain on palpation would indicate an alternate diagnosis.[1] Lateral hip pain reproduced on 30s single-leg stance test was a sensitivity and specificity of 100% and 97.3% respectively for gluteal tendinopathy.[1] The high utility of the test is only maintained if lateral displacement of the hip is avoided.[1] The examiner may provide gentle fingertip support to steady the patient.[1] The FABER test is useful in the differential diagnosis as limited range of movement is associated with hip joint pathology but not gluteal tendinopathy.[1] The Ober's test has been shown to lack diagnostic utility for gluteal tendinopathy.[1]
Investigations
MRI is gold standard as it can visualise changes associated with gluteal tendinopathy, such as tendon thickening and soft tissue oedema, the clearest.[1] MRI is also useful in excluding other causes of lateral hip pain.[1] However, MRI is expensive and not very accessible.[1] Consequently, ultrasound is typically used in clinical practice.[1] The accuracy of ultrasound in identifying gluteal tendinopathy is variable and dependent on operator experience and patient characteristics.[1] It is important to note that it is normal for radiological changes to be present in the asymptomatic population, thus, any findings need to be considered within the clinical context.[1]
Imaging Findings
Grey scale Ultrasound[4]
- Thickened tendons
- Reduced echogenicity of tendons
- More heterogeneous echogenicity of tendons
- Increased echogenicity of muscles as reduced muscle bulk and increased fat
- Partial tear are indicated by thinning of the tendon and partial thickness area free from echo
- Complete tear indicated by the full thickness of the tender being free from echo and a “bald” facet
- Deep to gluteus tendons insertions there may be cortical irregularities
On Doppler Ultrasound can helpfully but uncommonly see increased vascularity[4]
MRI[5]
- Intensity of signal increased in T1w view within tendons of gluteus minimus and/or gluteus medius
- Hyperintensity in T2 view within tendon of gluteus minimus and/or gluteus medius
- Presence of fluid distension of the greater trochanteric bursa
- On coronal T1w view, fatty streaks or fatty infiltration of gluteus minimus and/or gluteus medius
- Partial tear indicated by hyperintensity in T2 view within tendon of gluteus minimus and/or gluteus medius
- Partial tear can presents with or without tendon thinning
- Complete tear indicated by disruption of tendon of gluteus minimus and/or gluteus medius
- Osseous avulsion may or may not be present in a complete tear
Other Investigations
Other imaging techniques are currently being developed. These include ultrasound tissue characterisation and elastography.[1]
Diagnosis
No clear diagnostic criteria exists for gluteal tendinopathy.[6] Typically the diagnosis is made clinically.[6] The history most commonly involves lateral hip pain that is exacerbated by activity and lying on the affected side.[6] On examination, one would expect to find tenderness on palpation of the greater trochanter.[6] This is the most common clinical finding in gluteal tendinopathy.[6]
Hip osteoarthritis is a common differential diagnosis for lateral hip pain. Asking about difficulty in manipulating shoes and socks is a useful way to differentiate the conditions.[7] A paper published in the British Journal of Sports Medicine suggested that diagnostic criteria for gluteal tendinopathy should include the patient reporting to have no difficulty in manipulating socks and shoes.[7] This paper also suggested the diagnostic criteria to include lateral hip pain reproduced on the FABER test as the FABER test should not produce lateral hip pain in hip osteoarthritis.[7]
Differential Diagnosis
Treatment
Gluteal tendinopathy for the majority is self limiting.[6] It has been reported that more than 90% of people are responsive to conserverative treatment.[6] Those who are not are considered refractory cases.[6]
Conservative treatment can include physiotherapy, shockwave therapy, NSAIDs, corticosteroid injections (CSI) and PRP injections.[6] There are varying levels of evidence for each of these interventions. Evidence does not support the conservative treatment of deep transverse friction massage, therapeutic ultrasound and acupuncture.[6]
Physiotherapy that is based around eccentric exercises has been shown to be effective in other tendinopathies.[6] Therefore, eccentric exercise has promise in the treatment of gluteal tendinopathy.
Ultrasound can be used for needle guidance of CSI. The injectate is deposited directly on the bone and around the injections or into the tendon itself. However, no significant difference between ultrasound guided and blind injection outcomes have been found.[6] CSI may provide benefit in the short term but with a high recurrence rate and poorer results in the long term.
Given the paucity of treatments for chronic gluteal tendinopathy (>3 months) and transient amelioration effect of CSI, there is interest whether biologic products such as PRP may provide better long-term outcomes for this condition.[8] The use of PRP has been controversial, especially in tendinopathies given its slower onset of action to see its efficacy. Some tendons respond differently to PRP. Technician skills, type of condition being treated and type of PRP used are all variables that can affect its effectiveness.
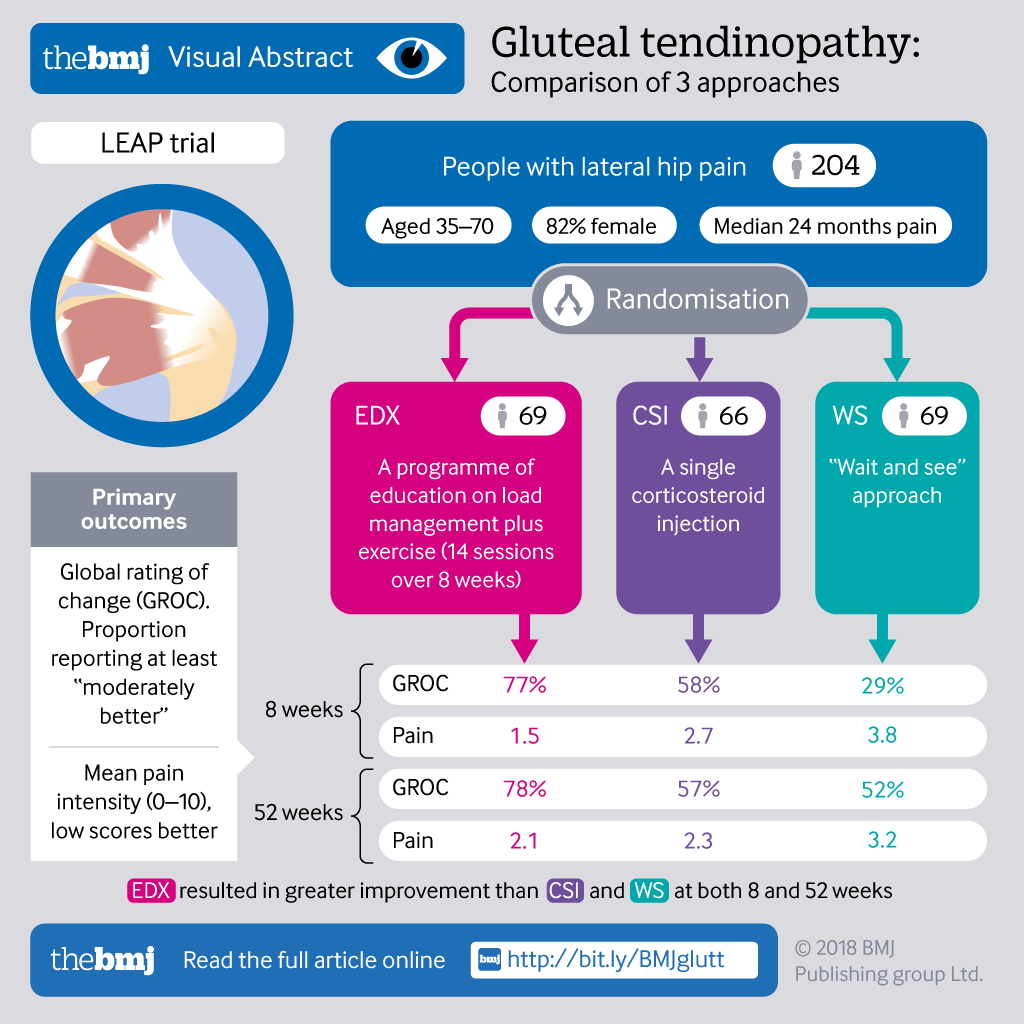
There is no universally prescribed treatment protocol.[6] However, the LEAP protocol is shown to be promising when compared to no treatment and single corticosteroid injection. The LEAP protocol involves education on load management (e.g. avoiding lying on side of affected leg) and a specific exercise programme. This study and its results can be found in the resources below.
Activity Modification
Avoid compression.
Exercise
Leap Trial
Surgery
Gluteal tendon reconstruction is experimental with no standardised techniques.[8]
Follow Up and Prognosis
Large number of patients fail non-operative treatment with significant levels of dysfunction making important to find novel treatment strategies.
Summary
Downloads
Links
How physiotherapists treat gluteal tendinopathy by Dr Alison Grimaldi
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 1.14 1.15 1.16 1.17 1.18 1.19 1.20 1.21 1.22 1.23 1.24 1.25 Grimaldi, Alison; Mellor, Rebecca; Hodges, Paul; Bennell, Kim; Wajswelner, Henry; Vicenzino, Bill (2015-05-13). "Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management". Sports Medicine. 45 (8): 1107–1119. doi:10.1007/s40279-015-0336-5. ISSN 0112-1642.
- ↑ 2.0 2.1 2.2 2.3 Cook, J L; Purdam, C R (2008-09-23). "Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy". British Journal of Sports Medicine. 43 (6): 409–416. doi:10.1136/bjsm.2008.051193. ISSN 0306-3674.
- ↑ Segal, Neil A.; Torner, James; Xie, Hui; Felson, David; Curtis, Jeffrey R.; Nevitt, Michael (2006-11-01). "PR_092: Greater Trochanteric Pain Syndrome: Epidemiology and Associated Factors". Archives of Physical Medicine and Rehabilitation (in English). 87 (11): e20. doi:10.1016/j.apmr.2006.08.114. ISSN 0003-9993.
- ↑ 4.0 4.1 Kong, Andrew; Van der Vliet, Andrew; Zadow, Steven (2006-12-06). "MRI and US of gluteal tendinopathy in greater trochanteric pain syndrome". European Radiology. 17 (7): 1772–1783. doi:10.1007/s00330-006-0485-x. ISSN 0938-7994.
- ↑ Dadour, Joseph Rudy; Gilbert, Guillaume; Lepage-Saucier, Marianne; Freire, Véronique; Bureau, Nathalie J. (2021-04-29). "Quantitative MRI in patients with gluteal tendinopathy and asymptomatic volunteers: initial results on T1- and T2*-mapping diagnostic accuracy and correlation with clinical assessment". Skeletal Radiology. 50 (11): 2221–2231. doi:10.1007/s00256-021-03781-0. ISSN 0364-2348.
- ↑ 6.00 6.01 6.02 6.03 6.04 6.05 6.06 6.07 6.08 6.09 6.10 6.11 6.12 Reid, Diane (2016-03). "The management of greater trochanteric pain syndrome: A systematic literature review". Journal of Orthopaedics. 13 (1): 15–28. doi:10.1016/j.jor.2015.12.006. ISSN 0972-978X. Check date values in:
|date=(help) - ↑ 7.0 7.1 7.2 Fearon, Angela M; Scarvell, Jennie M; Neeman, Terry; Cook, Jill L; Cormick, Wes; Smith, Paul N (2013-07). "Greater trochanteric pain syndrome: defining the clinical syndrome". British Journal of Sports Medicine (in English). 47 (10): 649–653. doi:10.1136/bjsports-2012-091565. ISSN 0306-3674. Check date values in:
|date=(help) - ↑ 8.0 8.1 Koulischer, Simon; Callewier, Antoine; Zorman, David (June 2017). "Management of greater trochanteric pain syndrome : a systematic review". Acta Orthopaedica Belgica. 83 (2): 205–214. ISSN 0001-6462. PMID 30399983.
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,


{kind=link}