Lumbar Medial Branch Blocks: Difference between revisions
No edit summary |
|||
| (3 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{Authors}} | {{Authors | ||
|Authors=Jeremy | |||
}} | |||
{{Procedure | {{Procedure | ||
|quality= | |quality=Partial | ||
|image=Lumbar medial branch blocks fluoroscopy left L3-5.jpg | |image=Lumbar medial branch blocks fluoroscopy left L3-5.jpg | ||
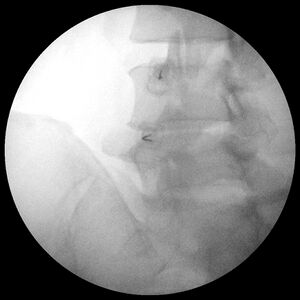
|caption=AP fluoroscopy image of left L3 and L4 medial branch and L5 dorsal ramus blocks. | |caption=AP fluoroscopy image of left L3 and L4 medial branch and L5 dorsal ramus blocks. | ||
| Line 7: | Line 9: | ||
|syringe=3mL syringe | |syringe=3mL syringe | ||
|needle=22-25g 3.5 inch spinal needle with a bent tip | |needle=22-25g 3.5 inch spinal needle with a bent tip | ||
|steroid=Not appropriate | |||
|local=1-4% lidocaine or 0.5-0.75% bupivacaine | |local=1-4% lidocaine or 0.5-0.75% bupivacaine | ||
|volume=0.5mL over each targeted nerve | |volume=0.5mL over each targeted nerve | ||
}} | |||
Controlled lumbar medial branch and L5 dorsal ramus blocks are the only validated tool for diagnosing [[Lumbar Zygapophysial Joint Pain|lumbar zygapophysial joint pain]]. | Controlled lumbar medial branch and L5 dorsal ramus blocks are the only validated tool for diagnosing [[Lumbar Zygapophysial Joint Pain|lumbar zygapophysial joint pain]]. | ||
== Anatomy == | ==Anatomy== | ||
Each zygapophysial joint is innervated by two nerves and so both need to be anaesthetised. At the L1-4 neural segments the target is the medial branch of the dorsal ramus. At the L5 neural segment the target is the L5 dorsal ramus. The medial branches at each level are located at the junction of the superior articular process (SAP) and transverse process (TP) of the level below. The L5 dorsal ramus is at the junction of the S1 SAP and sacral ala. The L4 medial branch is found at the junction (jx) of the L5 SAP and TP, etc. | Each zygapophysial joint is innervated by two nerves and so both need to be anaesthetised. At the L1-4 neural segments the target is the medial branch of the dorsal ramus. At the L5 neural segment the target is the L5 dorsal ramus. The medial branches at each level are located at the junction of the superior articular process (SAP) and transverse process (TP) of the level below. The L5 dorsal ramus is at the junction of the S1 SAP and sacral ala. The L4 medial branch is found at the junction (jx) of the L5 SAP and TP, etc. | ||
{| class="wikitable" | {| class="wikitable" | ||
| Line 33: | Line 36: | ||
The medial branches run at what is called the "inflexion" which is the curve between the base of the SAP and the upper border of the TP and the mamillo-accessory ligament. There is no mamillo-accessory ligament at S1. The mamillo-accessory ligament passes between the mamillary process on the base of the superior articular process and the accessory process on the proximal end of the transverse process. | The medial branches run at what is called the "inflexion" which is the curve between the base of the SAP and the upper border of the TP and the mamillo-accessory ligament. There is no mamillo-accessory ligament at S1. The mamillo-accessory ligament passes between the mamillary process on the base of the superior articular process and the accessory process on the proximal end of the transverse process. | ||
== Indications == | ==Indications== | ||
The indication is [[Chronic Low Back Pain|chronic low back pain]] that is not responding to conservative management to assess whether the pain is arising from one or more lumbar zygapophysial joints. Positive blocks can lead to the validated treatment option of [[Lumbar Zygapophysial Joint Precision Treatment|radiofrequency neurotomy]]. It is the primary test in the older patient where zygapophysial joints may account for 40% of axial pain. In younger patients zygapophysial joint pain is usually only considered when discogenic pain has been excluded. | The indication is [[Chronic Low Back Pain|chronic low back pain]] that is not responding to conservative management to assess whether the pain is arising from one or more lumbar zygapophysial joints. Positive blocks can lead to the validated treatment option of [[Lumbar Zygapophysial Joint Precision Treatment|radiofrequency neurotomy]]. It is the primary test in the older patient where zygapophysial joints may account for 40% of axial pain. In younger patients zygapophysial joint pain is usually only considered when discogenic pain has been excluded. | ||
| Line 50: | Line 53: | ||
===L1-L4 Medial Branches=== | ===L1-L4 Medial Branches=== | ||
*Preparation | |||
**Position: Patient is prone with a pillow under their abdomen in order to decrease the lordosis. | |||
**Prep and drape | |||
*Target visualisation | |||
**Under fluoroscopy first evaluate the lumbosacral region for transitional anatomy | |||
**Palpate the spine to find the level to be tested. Use maximal point tenderness. | |||
**Position the C-arm so that the target vertebra is in the middle | |||
**"Square off" the superior endplate. This refers to tilting the C-arm cephalo-caudally so that the beam is parallel to the endplate. For example if the target is the L4 medial branch at L5 then square off the superior endplate of L5 | |||
**Rotate the C-arm ipsilaterally to obtain an oblique view. Visualise the inflexion point between the SAP and TP, usually this is at about 40 degrees. | |||
**The target is approximately 1/3 to 1/2 the distance between the inflexion and mamillary process. | |||
*Needle placement | |||
**Optional local anaesthetic intradermally | |||
**Insert spinal needle slightly lateral to target, go down the beam, and advance until bone is contacted | |||
**Confirm needle position in AP view. The needle tip should be located right at or slightly medial to the lateral margin of the SAP | |||
**Use a decline view to confirm needle tip location. The tip should point into the notch located between the SAP and TP. | |||
**If there is concern about depth an inadvertent entry into the foramen then obtain a lateral view | |||
**Twist needle so that the bevel faces medially | |||
*Injection | |||
**Connect a low volume extension tube to the syringe | |||
**Contrast: inject 0.1-0.3 mL of contrast under live fluoroscopy. Observe for aberrant flow especially venous uptake which can lead to a false negative. The contrast should cover the path of the medial branch. The decline view can again be used to confirm spread. | |||
**Inject 0.3-0.5mL of local anaesthetic | |||
<gallery widths=300px heights=300px> | |||
File:MBB Left L3 and L4 Oblique.jpg|Needle entry via ipsilateral oblique route targeting left L3 and L4 medial branches. | |||
File:MBB Left L3 and L4 Decline.jpg|Needle location decline view | |||
File:MBB Left L3 and L4.jpg|Needle location AP view | |||
File:MBB Left L3 and L4 AP contrast.jpg|Contrast spread | |||
</gallery> | |||
===L5 Dorsal Ramus=== | |||
=== L5 Dorsal Ramus === | |||
As above but the inflexion is between the S1 SAP and sacral ala. There is no shadow of the SAP. The L% dorsal ramus is found in the bony groove at the base of hte S1 SAP. The target region is 1/3 to 1/2 along the course of the L5 dorsal ramus between the inflexion and base of the L5/S1 zygapophysial joint. | As above but the inflexion is between the S1 SAP and sacral ala. There is no shadow of the SAP. The L% dorsal ramus is found in the bony groove at the base of hte S1 SAP. The target region is 1/3 to 1/2 along the course of the L5 dorsal ramus between the inflexion and base of the L5/S1 zygapophysial joint. | ||
| Line 79: | Line 87: | ||
==Post-Procedural Evaluation== | ==Post-Procedural Evaluation== | ||
The patient should be evaluated 30 | The patient should be evaluated immediately post block (10 minutes), 30 minutes after the block, hourly for the first 4 hours, and the next day. It is ideal if the evaluator is independent and also blinded to the anaesthetic used. | ||
Document any neurological deficit of the lower extremity. | Document any neurological deficit of the lower extremity. | ||
| Line 85: | Line 93: | ||
A positive test requires close to 100% relief of the index pain with provocative movement. 80% relief may be considered when residual pain is <1/10. | A positive test requires close to 100% relief of the index pain with provocative movement. 80% relief may be considered when residual pain is <1/10. | ||
A 30% false positive rate is seen, and so controlled blocks are required prior to undertaking [[Lumbar Zygapophysial Joint Precision Treatment|radiofrequency neurotomy]]. | A 30% false positive rate is seen, and so controlled blocks are required prior to undertaking [[Lumbar Zygapophysial Joint Precision Treatment|radiofrequency neurotomy]]. Using single blocks only 47% have >50% relief of pain (mean duration 9.9 months), while using double-blocks 77% have >50% relief of pain.<ref>{{Cite journal|last=Derby|first=Richard|last2=Melnik|first2=Irina|last3=Lee|first3=Jeong-Eun|last4=Lee|first4=Sang-Heon|date=2012-12|title=Correlation of lumbar medial branch neurotomy results with diagnostic medial branch block cutoff values to optimize therapeutic outcome|url=https://pubmed.ncbi.nlm.nih.gov/23126379|journal=Pain Medicine (Malden, Mass.)|volume=13|issue=12|pages=1533–1546|doi=10.1111/j.1526-4637.2012.01500.x|issn=1526-4637|pmid=23126379}}</ref> | ||
===Possible Responses=== | |||
'''Concordant response''': longer pain relief from bupivacaine than from lidocaine. This is a true positive response. | |||
'''Concordant prolonged response''': longer pain relief from bupivacaine than from lidocaine but prolonged pain relief. This is also considered a true positive response. The reason for prolonged relief could be from intra-neural injection, transection of target nerve, or or as yet undescribed mechanisms. | |||
'''Discordant response''': longer relief from lidocaine than bupivacaine. This is considered a negative response. | |||
'''Discrepant''': Relief from the first but not second block. The most likely reason is that the joint is not the source of pain. Other possibilities is that one procedure used an incorrect technique or that the patient is unreliable. | |||
'''Negative''': No relief from blocks. | |||
===Criteria=== | |||
There are two criteria that can be used. | |||
'''Stringent criteria:''' this is when only concordant responses are considered positive. The advantages of this is that it increases the success rate of RF, reduces the demand on RF, but it can deny treatment to some patients that may benefit. | |||
'''Expanded criteria''': This is when concordant and discordant responses are considered positive. The advantage is that no patients are incorrectly denied RF, but it means that some patients get RF that won't benefit, and it prolongs the waitlist. | |||
== References == | ==Resources== | ||
{{Members link}} | |||
==References== | |||
[[Category:Lumbar Spine Procedures]] | [[Category:Lumbar Spine Procedures]] | ||
<references /> | |||
Latest revision as of 13:59, 15 April 2022

| |
| Lumbar Medial Branch Blocks | |
|---|---|
| Indication | Diagnostic test for Lumbar Zygapophysial Joint Pain |
| Syringe | 3mL syringe |
| Needle | 22-25g 3.5 inch spinal needle with a bent tip |
| Steroid | Not appropriate |
| Local | 1-4% lidocaine or 0.5-0.75% bupivacaine |
| Volume | 0.5mL over each targeted nerve |
Controlled lumbar medial branch and L5 dorsal ramus blocks are the only validated tool for diagnosing lumbar zygapophysial joint pain.
Anatomy
Each zygapophysial joint is innervated by two nerves and so both need to be anaesthetised. At the L1-4 neural segments the target is the medial branch of the dorsal ramus. At the L5 neural segment the target is the L5 dorsal ramus. The medial branches at each level are located at the junction of the superior articular process (SAP) and transverse process (TP) of the level below. The L5 dorsal ramus is at the junction of the S1 SAP and sacral ala. The L4 medial branch is found at the junction (jx) of the L5 SAP and TP, etc.
| Joint | Inferior innervation | Superior innervation |
|---|---|---|
| L5/S1 facet joint | L5 dorsal ramus at S1 jx SAP and sacral ala | L4 medial branch at L5 jx SAP and TAP |
| L4/5 facet joint | L4 medial branch at L5 jx SAP and TP | L3 medial branch at L4 jx SAP and TAP |
| L3/4 facet joint | L3 medial branch at L4 jx SAP and TAP | L2 medial branch at L3 jx SAP and TAP |
The medial branches run at what is called the "inflexion" which is the curve between the base of the SAP and the upper border of the TP and the mamillo-accessory ligament. There is no mamillo-accessory ligament at S1. The mamillo-accessory ligament passes between the mamillary process on the base of the superior articular process and the accessory process on the proximal end of the transverse process.
Indications
The indication is chronic low back pain that is not responding to conservative management to assess whether the pain is arising from one or more lumbar zygapophysial joints. Positive blocks can lead to the validated treatment option of radiofrequency neurotomy. It is the primary test in the older patient where zygapophysial joints may account for 40% of axial pain. In younger patients zygapophysial joint pain is usually only considered when discogenic pain has been excluded.
Pre-Procedural Evaluation
Obtain adequate consent. An emphasis should be placed on this procedure being a test not a treatment. This concept should be repeated several times and also be provided in written information. The concept can be reinforced through visual means by drawing a pain graph for the patient showing the expected response with pain going back up to baseline. Despite all this some patients may still be surprised that the pain came back after the anaesthetic wears off.
Appropriate target(s) should be selected. The majority of positive cases are found to be single level and unilateral. Injections of >2 levels and routine bilateral injections are not supported.
Premedication is not recommended because it can interfere with the interpretation of the results. If the patient cannot tolerate the procedure without premedication due to anxiety then the anxiety should be treated first rather than proceeding to medial branch blocks.
No physiological monitoring or intravenous access is required.
Before the procedure the patient records a pain diagram, their pain ratings (worst ever experienced, worst ever for index pain, and index pain on day of procedure), and four activities that are limited by the index pain. The recording sheet has a section for recording the pain before, immediately following, and several hours after the procedure, along with an area for recording whether painful activities are restored.
Technique
L1-L4 Medial Branches
- Preparation
- Position: Patient is prone with a pillow under their abdomen in order to decrease the lordosis.
- Prep and drape
- Target visualisation
- Under fluoroscopy first evaluate the lumbosacral region for transitional anatomy
- Palpate the spine to find the level to be tested. Use maximal point tenderness.
- Position the C-arm so that the target vertebra is in the middle
- "Square off" the superior endplate. This refers to tilting the C-arm cephalo-caudally so that the beam is parallel to the endplate. For example if the target is the L4 medial branch at L5 then square off the superior endplate of L5
- Rotate the C-arm ipsilaterally to obtain an oblique view. Visualise the inflexion point between the SAP and TP, usually this is at about 40 degrees.
- The target is approximately 1/3 to 1/2 the distance between the inflexion and mamillary process.
- Needle placement
- Optional local anaesthetic intradermally
- Insert spinal needle slightly lateral to target, go down the beam, and advance until bone is contacted
- Confirm needle position in AP view. The needle tip should be located right at or slightly medial to the lateral margin of the SAP
- Use a decline view to confirm needle tip location. The tip should point into the notch located between the SAP and TP.
- If there is concern about depth an inadvertent entry into the foramen then obtain a lateral view
- Twist needle so that the bevel faces medially
- Injection
- Connect a low volume extension tube to the syringe
- Contrast: inject 0.1-0.3 mL of contrast under live fluoroscopy. Observe for aberrant flow especially venous uptake which can lead to a false negative. The contrast should cover the path of the medial branch. The decline view can again be used to confirm spread.
- Inject 0.3-0.5mL of local anaesthetic
Needle entry via ipsilateral oblique route targeting left L3 and L4 medial branches.

Needle location decline view

Needle location AP view

Contrast spread




L5 Dorsal Ramus
As above but the inflexion is between the S1 SAP and sacral ala. There is no shadow of the SAP. The L% dorsal ramus is found in the bony groove at the base of hte S1 SAP. The target region is 1/3 to 1/2 along the course of the L5 dorsal ramus between the inflexion and base of the L5/S1 zygapophysial joint.
The iliac crests can overlap and obscure the target region in the oblique view. There are two options to overcome this. One is to reduce the obliquity and use a curved needle to move around the SAP bulge. The other option is to tilt the C-arm further cephalad which will move the iliac crests caudally.
Post-Procedural Evaluation
The patient should be evaluated immediately post block (10 minutes), 30 minutes after the block, hourly for the first 4 hours, and the next day. It is ideal if the evaluator is independent and also blinded to the anaesthetic used.
Document any neurological deficit of the lower extremity.
A positive test requires close to 100% relief of the index pain with provocative movement. 80% relief may be considered when residual pain is <1/10.
A 30% false positive rate is seen, and so controlled blocks are required prior to undertaking radiofrequency neurotomy. Using single blocks only 47% have >50% relief of pain (mean duration 9.9 months), while using double-blocks 77% have >50% relief of pain.[1]
Possible Responses
Concordant response: longer pain relief from bupivacaine than from lidocaine. This is a true positive response.
Concordant prolonged response: longer pain relief from bupivacaine than from lidocaine but prolonged pain relief. This is also considered a true positive response. The reason for prolonged relief could be from intra-neural injection, transection of target nerve, or or as yet undescribed mechanisms.
Discordant response: longer relief from lidocaine than bupivacaine. This is considered a negative response.
Discrepant: Relief from the first but not second block. The most likely reason is that the joint is not the source of pain. Other possibilities is that one procedure used an incorrect technique or that the patient is unreliable.
Negative: No relief from blocks.
Criteria
There are two criteria that can be used.
Stringent criteria: this is when only concordant responses are considered positive. The advantages of this is that it increases the success rate of RF, reduces the demand on RF, but it can deny treatment to some patients that may benefit.
Expanded criteria: This is when concordant and discordant responses are considered positive. The advantage is that no patients are incorrectly denied RF, but it means that some patients get RF that won't benefit, and it prolongs the waitlist.
Resources
References
- ↑ Derby, Richard; Melnik, Irina; Lee, Jeong-Eun; Lee, Sang-Heon (2012-12). "Correlation of lumbar medial branch neurotomy results with diagnostic medial branch block cutoff values to optimize therapeutic outcome". Pain Medicine (Malden, Mass.). 13 (12): 1533–1546. doi:10.1111/j.1526-4637.2012.01500.x. ISSN 1526-4637. PMID 23126379. Check date values in:
|date=(help)

