


- Neuronopathies
- Thoracic Hyperkyphosis
- Developmental Dysplasia of the Hip
- Shin Pain
- Post-Inguinal Hernia Repair Chronic Pain
- Ilioinguinal and Iliohypogastric Nerve Injection
- Channelopathies and Chronic Pain
- Tricyclic Antidepressants
- Parkinson's Disease and Chronic Pain
- Carbamazepine
- Paroxysmal Extreme Pain Disorder
- Fascia
- Lumbar Spine Arthrodesis
- Lumbar Pseudoarthrosis
- Patient Reported Outcome Measures
- Fabry Disease
- Notalgia Paraesthetica
- Erythromelalgia
- Sodium Channelopathies
- Myotonia
Main Page
From WikiMSK
WELCOME TO WIKIMSK
The New Zealand Musculoskeletal Medicine Wiki
Nau mai, haere mai! This website is a learning resource that is primarily designed for Musculoskeletal Medicine training in New Zealand. It also aims to be useful for GPs, other doctors, and medical students. It is not written for patients but they are welcome to read the articles. Click on a body region on the skeleton or a portal below to get started.

Featured Wiki Article for 1 July 2023
Referred Pain
Referred pain is best described in neurological terms as "pain perceived as arising or occurring in a region of the body innervated by nerves or branches of nerves other than those that innervate the actual source of pain" (IASP definition). In topographical terms it is perceived in a region that is topographically distinct from the actual source of the pain. The topographical definition becomes ambiguous in cases where it is unclear where one region of the body ends and an adjacent region begins. Referred pain is a very common presentation of pain. For pain in a particular area, the diagnostic process should start by asking which body segment are they indicating, and then translate that into which structures are supplied by those spinal cord segments. - Read More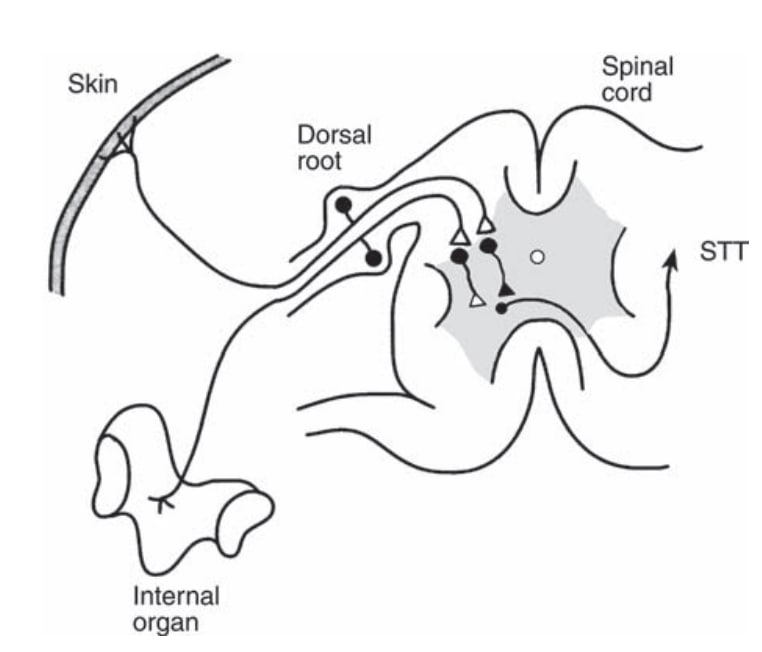
New and Updated Articles
- Hip Joint Injection
- Vertigo and Dizziness
- Thoracic Hyperkyphosis
- Lateral Elbow Tendinopathy
- Dermatomes
- Smoking and Chronic Pain
- Distal Clavicle Osteolysis
- Neuronopathies
- Neuromuscular Disorders Overview
- Sensory Polyneuropathies
- Developmental Dysplasia of the Hip
- Idiopathic Scoliosis
- Hip Osteoarthritis
- Shin Pain
- Medial Tibial Stress Syndrome
- Coccydynia
- Adult Acquired Flatfoot Deformity
- Orthoses for Neurological Ankles
- Transitional Vertebral Anatomy
- Gabapentinoids
Featured Open Access Journal Article for 1 June 2023
On the validity and clinical utility of comparative local anesthetic blocks for the diagnosis of spine pain
Interventional Pain Medicine
ABSTRACT - This comprehensive review article revisits the validity and utility of comparative local anesthetic blocks, specifically in the diagnosis of spine pain. These blocks have provided an effective alternative to placebo controls. The discussion includes biostatistical principles involved in assessing the validity and clinical utility of diagnostic tests in relation to existing empirical studies. The review refutes recent claims questioning the clinical utility of these blocks, and highlights the need for studies that correctly test and compare the durations of action of the two anesthetic agents. It concludes that the validity of diagnostic tests is measured by likelihood ratios, and the clinical utility is measured by the diagnostic confidence provided by these likelihood ratios according to the prevalence of the condition being diagnosed.
“I will respect the hard-won scientific gains of those physicians in whose steps I walk, and gladly share such knowledge as is mine with those who are to follow.”
— The Hippocratic Oath: Modern Version, Lasagna 1964

