Referred Pain
Referred pain is pain perceived in a region innervated by nerves different from those that innervate the actual source of pain. Referred pain is probably the most common presentation of pain.
Ascending Pathways
The pathways of stimuli coming from skin ascend up the spinal cord largely through the spinothalamic tract for noxious stimuli, and the posterior columns for tactile stimuli, and thence through to the thalamus. Different types of information is recorded by different pathways. This multiplicity endows skin stimuli with good localisation in the thalamus and the cerebral cortex. The ability to localise skin stimuli if the posterior columns are interrupted. There is good somatotopic organisation with a faithful continuation of representation of points in the skin to particular cells in the pathways.
In contrast, stimuli from deep structures such as bones, ligaments, joints, and muscles have a fairly restricted pathway largely through the spinothalamic tract, but also through collaterals into the reticular formation of the brainstem constituting the spinoreticulothalamic tract (SRTT). In this system there are a large number of neurons with several synapses and connections along the pathway. This system has poor somatotopic organisation.
In an evolutionary sense, there is no point in having an expensive highly localised sensory system for deep structures because unlike with the skin, there is nothing that the organism can do about pain in deep areas.
Convergence

In systems like the STT pathways that is relatively predominant in the innervation of deep structures, neurons are used economically. Two nerves in the periphery might converge on a single neuron. The axons of two of those neurons may converge on yet another single neuron, and so on. This pattern of converge is seen throughout the pathway: between primary afferent and cells in the spinal cord, between cells from the spinal card into the higher nuclei, and then onto the thalamus.
The frontal lobe therefore has no way of knowing which exact cell the stimuli originated from. In general the thalamus knows the location within plus or minus one spinal cord segment. In contrast to knowing a specific area of the big toe, it thinks the information is arising from around L5, but maybe L4 or S1.
Body Segments
Some authors state that referred pain occurs in dermatomes. This is neither an appropriate or accurate model for referred pain. There is no reliable or accurate relationship between the area of referred pain and the dermatome that seems to cover it. Therefore avoid describing referred pain in terms of dermatomal patterns. The term that is best applied is that of a body segment.
The simplest arrangement is the trunk with definable anatomical segments. Each segments has a rib, ligaments, muscles, (and skin). The limbs are a lot more complicated. Each intercostal nerve supplies the segment through which it runs. The nerves can be followed from the back around to the front. The upper thoracic nerves stay in their intercostal spaces and travel towards the sternum. The T6-L1 nerves pass across the costal margin, away from the sternum largely following the direction of the bones but not the costal cartilages, and into the abdominal region. They continue to supply the muscles and tissues in those bands. L2 and lower are distributed to the lower limbs.
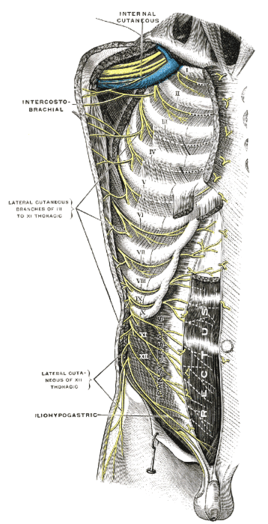
Intercostal nerves
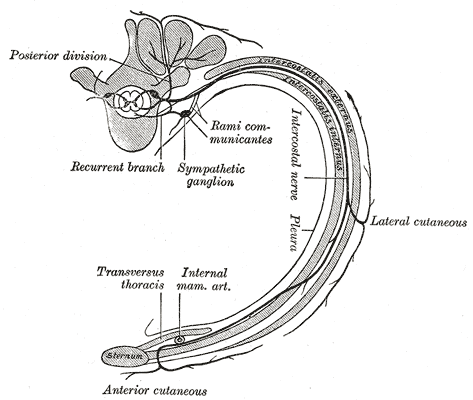
The course and branches of a typical intercostal nerve



