Dermatomes: Difference between revisions
No edit summary |
No edit summary |
||
| Line 16: | Line 16: | ||
File:dermatome map Keegan and garrett.png|Keegan and Garrett 1948 - Hypoalgesia secondary to nerve root compression | File:dermatome map Keegan and garrett.png|Keegan and Garrett 1948 - Hypoalgesia secondary to nerve root compression | ||
</gallery> | </gallery> | ||
{| class="wikitable" | |||
|- | |||
! Authors !! Year !! Basis of Map !! Findings !! Weaknesses | |||
|- | |||
| Herringham || 1886 || The first account of the distribution of segmental nerve fibres into the upper limb based on dissection || Axial line. The dermatomes in the preaxial area (C5-6) are higher than those in the post axial area (C8-T1). In the preaxial area the forearm (C6) is supplied by a lower nerve than the arm (C5), in the post axial area the forearm (C8) is supplied by a higher nerve than the arm (T1-2)||Only based on dissection and theory. | |||
|- | |||
| Head and Campbell || 1900 || Zoster eruptions in 450 patients, with histological confirmation in some subjects. || Noted some overlap, changed with body shape and age. || Histological confirmation in only 16 cases. No examples of C8 or S1. Assumptions were made about the exact dorsal root involved. Herpetic eruptions can affect several adjacent levels. Not all cutaneous fibres will necessarily be infected. | |||
|- | |||
| Fender and Foerster || 1933 and 1936 || Residual area of sensation after surgically isolating single dorsal nerve roots. L1 to S2 isolated by dividing nerve roots above and below the target level. Cervical dermatomes mostly assessed by dividing nerve roots either above or below thus obtaining proximal and distal boundaries only. Vasodilation following electrical stimulation supplemented the data. Population those with spasticity (mostly those with tabes dorsalis).|| Areas vary between individuals, except in the midline. Tactile dermatomes are larger than those determined by pain and temperature. With the exception of C2 there is no sensory loss if only one nerve root is sectioned. || Relatively few subjects, poorly documented methods and testing protocol, no information about time interval between sectioning and testing. | |||
|} | |||
==Videos== | ==Videos== | ||
Revision as of 06:43, 15 August 2020
The most up to date dermatome map is probably that published by Lee et al. They created a composite image taken from published data that they thought was the most reliable. [1] The winding band like dermatomal map seen in some textbooks was from Keegan and Garrett is the most flawed of all dermatomal maps and was not included. Lee et al's map is most consistent tactile dermatomal regions for each spinal dorsal nerve root. The midline has minimal overlap, but otherwise there is extensive and variable overlap. Blank areas on the map represent areas where there is very large degree of variability and overlap. The S3, S4, and S5 cutaneous supply is not shown.

Radicular pain does not necessarily follow dermatomal distribution.[2]
History
See Downs et al on the history of dermatome maps.[3]

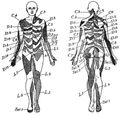
Herringham 1886 - Dissection and theory
Sherington 1893 - Severing dorsal nerve roots in monkeys
Head and Campbell 1900 - Zoster eruptions

Fender after Foerster lower body 1933 and 1936 - sensation after surgical resection of adjacent roots

Fender after Foerster upper body 1933 and 1936 - sensation after surgical resection of adjacent roots

Keegan and Garrett 1948 - Hypoalgesia secondary to nerve root compression





| Authors | Year | Basis of Map | Findings | Weaknesses |
|---|---|---|---|---|
| Herringham | 1886 | The first account of the distribution of segmental nerve fibres into the upper limb based on dissection | Axial line. The dermatomes in the preaxial area (C5-6) are higher than those in the post axial area (C8-T1). In the preaxial area the forearm (C6) is supplied by a lower nerve than the arm (C5), in the post axial area the forearm (C8) is supplied by a higher nerve than the arm (T1-2) | Only based on dissection and theory. |
| Head and Campbell | 1900 | Zoster eruptions in 450 patients, with histological confirmation in some subjects. | Noted some overlap, changed with body shape and age. | Histological confirmation in only 16 cases. No examples of C8 or S1. Assumptions were made about the exact dorsal root involved. Herpetic eruptions can affect several adjacent levels. Not all cutaneous fibres will necessarily be infected. |
| Fender and Foerster | 1933 and 1936 | Residual area of sensation after surgically isolating single dorsal nerve roots. L1 to S2 isolated by dividing nerve roots above and below the target level. Cervical dermatomes mostly assessed by dividing nerve roots either above or below thus obtaining proximal and distal boundaries only. Vasodilation following electrical stimulation supplemented the data. Population those with spasticity (mostly those with tabes dorsalis). | Areas vary between individuals, except in the midline. Tactile dermatomes are larger than those determined by pain and temperature. With the exception of C2 there is no sensory loss if only one nerve root is sectioned. | Relatively few subjects, poorly documented methods and testing protocol, no information about time interval between sectioning and testing. |
Videos
- ↑ Lee et al.. An evidence-based approach to human dermatomes. Clinical anatomy (New York, N.Y.) 2008. 21:363-73. PMID: 18470936. DOI.
- ↑ Furman & Johnson. Induced lumbosacral radicular symptom referral patterns: a descriptive study. The spine journal : official journal of the North American Spine Society 2019. 19:163-170. PMID: 29800710. DOI.
- ↑ Downs & Laporte. Conflicting dermatome maps: educational and clinical implications. The Journal of orthopaedic and sports physical therapy 2011. 41:427-34. PMID: 21628826. DOI.

