Interspinous Oedema
| Interspinous Oedema | |
|---|---|
| Synonym | Interspinous bursitis, Baastrup Disease, kissing spines |
| Definition | Pain arising from oedema in the interspinous space |
| Epidemiology | Further research required |
| Causes | Trauma, rheumatological |
| Clinical Features | Pain closely linked to an accident, variable pain distribution, severe pain, tender interspinous space. |
| Tests | MRI and diagnostic injection |
| Treatment | Image guided interspinous space corticosteroid injection |
Interspinous oedema is a finding seen on MRI and can be symptomatic or asymptomatic. This finding is typically seen in the lumbar spine, but also occurs in the cervical spine.
Anatomy

There are several soft tissue structures located in the posterior aspect of the lumbar spines. Namely, the multifidi muscles, interspinalis muscles, interspinous ligaments, and fat. Some authors state that there are a variable number of bursae in the spinal column, that are normally located between the spinous processes of the cervical and lumbar segments. All the above structures, as well as the periosteum of the spinous processes, are innervated by the medial branches of the lumbar dorsal rami, the same innervation as the facet joints.
Aetiology

Interspinous oedema simply refers to a radiological finding, and does not presuppose any underlying cause. Bogduk theorises that the pain arises as a result of a periostitis of the spinous processes, or inflammation of the interspinous ligament, with nociception arising from the medial branches of the dorsal rami [1] Some authors use the term interspinous bursitis. The term bursitis, implying bursal pathology, is not able to be proven on imaging as the oedema could be from any number of causes. The term oedema is therefore preferred, although a bursal process is probably more likely in rheumatological cases. [2]
Interspinous oedema most commonly occurs in the mid and lower lumbar segments, and the finding increases in frequency with advancing age.[3]
Trauma In the experience of one Musculoskeletal Medicine Specialist, this is the most common cause (see epidemiology section). It mostly occurs by lifting in flexion and occasionally in hyperextension. It can also occur with a fall. The tissue injured is speculative but it is thought that the interspinous soft tissues are injured by compression between the bony spinous processes.[2] Strain can result in changes to the interspinous ligaments, and rupture of the supraspinous and interspinous ligaments can even occur, most commonly in women aged between 15-35.[3]
Some hypotheses:[2]
Injury in flexion when lifting, where there is eccentric load on the muscles. The multifidi cross several joints and that fits the usual mechanism of muscle sprain
- Reflex avlusion like a Jone's fracture of the base of the 5th metatarsal
- Sprain of the interspinous ligaments from excessive flexion
- Or a combination of the above
In a fall
- Sudden unguarded contraction of the interspinous muscles causing an avulsion
Asymptomatic/Incidental
Interspinous oedema can be an incidental finding, as evidenced by a negative response to a diagnostic local anaesthetic injection (see audit activity in epidemiology section).
Baastrup's Disease
Baastrup's and the synonym kissing spines should be reserved for when there is evidence of spinous process impaction. It has traditionally been thought that Baastrup's is due to excessive lumbar lordosis, but this has been refuted in an MRI study.[4] However but in this study, the authors used Baastrup's and interspinous oedema interchangeably, and did not differentiate between traumatic and atraumatic causes, nor did they differentiate whether there was lumbar spine impaction. In true Baastrup's the adjacent spinous processes, the most common level being L4/5, compresses the intervening interspinous ligament. It is more common in the degenerative lumbar spine in those aged 70 and older, with no gender predilection. The changes occur in the context of disc height loss, spondylolisthesis, and spondylosis.[5][1] The clinical relevance of this entity is not clear as one study found that surgical excision of the spinous processes was only successful in 11 out of 64 patients.[6]
Rheumatological Conditions
Interspinous bursitis has been associated with several rheumatological conditions, especially polymyalgia rheumatica (47% of RA patients), but also rheumatoid arthritis (10%), and crystalopathies. Lumbar spine involvement is more common than cervical spine, even though neck pain is more common than low back pain. Overall the relationship with pain in these patients is not clear, but in a control group the findings were only seen in 1 out of 65 patients.[7][8]
Epidemiology
A New Zealand Musculoskeletal Medicine Physician conducted an audit of their practice over 12-18 months from December 2019. The term symptomatic was applied when there was interspinous oedema on MRI and significant improvement with a fluoroscopically guided injection. Of 178 new cases of low back pain +/- leg pain, there were 21 cases of symptomatic interspinous oedema (12% prevalence), 6 cases of asymptomatic interspinous oedema (3.3% prevalence), and 10 inconclusive cases (5.6% prevalence)
An MRI study using of 539 patients with back or leg pain found lumbar interspinous bursitis to be present in 8.2% of cases. When present, it was seen at multiple levels in 47.7%; 71.4% of these cases had two levels involved, and 28.6% had 3 levels involved. The machine was 1.5 Tesla, fat suppression was not routinely used, and coronal sequences were not obtained. There was no control group, and no correlation with diagnostic blocks. The authors found an association with anterolisthesis and central spinal canal stenosis, and theorised that "bursitis" may develop due to translational movements of the spinous processes abutting each other. There was no association with lordosis.[4]
Clinical Features
- See also: Case:Low Back Pain 002
The clinical experience of one Musculoskeletal Medicine Physician has found certain patterns in the presentation. The onset of pain is closely linked to the time of the accident/forces. The patient is definite about the accident. The pain distribution is highly variable. The pain is significant, and affects sleep, work, and recreation. On examination there is tenderness of the interspinous soft tissues.
| Age | Duration of Pain | Injury | Interspace | Pain Drawing |
|---|---|---|---|---|
| 31 | 2 months | lifting and throwing concrete into skip bin | L4/5 | 
|
| 39 | 8 months | Lifting rail 'ping' | L4/5 L5/S1 | 
|
| 55 | 3 months | Fall | L4/5 | 
|
| 41 | 3 months | Lifting at gym | L4/5 L5/S1 | 
|
| 30 | 1 month | Lifting child | L5/S1 | 
|
| 65 | 11 months | Pulling out pallet which snagged | 
|
In kissing spines, patients may have midline back pain that worsens with extension and relieved by flexion. On examination the patient may be tender over the suspected level. Rarely an epidural cystic mass may cause neurogenic claudication with extension.[5]
Imaging


The diagnosis is supported by finding interspinous oedema on MRI. The two key sequences are the coronal fat sat Dixon and the T2 sagittal sequence. The coronal fat sat sequence needs to be specifically requested at certain radiology providers in New Zealand.
Kissing Spines
Imaging includes radiography, CT, and MRI. The hallmark finding suggestive of kissing spines is close approximation and contact of adjacent spinous processes with all the subsequent findings, including oedema, cystic lesions, sclerosis, flattening and enlargement of the articulating surfaces, bursitis and occasionally epidural cysts or midline epidural fibrotic masses.[5]
On x-rays, the most common finding is the close approximation and contact of adjacent spinous processes. There may be sclerosis of the articulating surfaces. In more severe cases, there is flattening and enlargement of the articulating surfaces or articulation of the two affected spinous processes. Usually generalised degenerative spinal changes are seen, most prominent at the affected level.[5]
CT shows close approximation and contact of the adjacent spinous processes. There is sclerosis, flattening, and enlargement of the articulating surfaces or the articulation of the two affected spinous processes. In rare cases there may be soft tissue nodules on the sides of the spinous process, and this could represent dissection of the spinal bursa superficial to the erector spinae. There are usually findings of degenerative changes such as facet joint hypertrophy, disc herniation, and spondylolisthesis.[5]
On MRI, under 10% of symptomatic patients have findings of interspinous bursitis. Bursitis appears as a fluid-like signal located between the two suspect spinous processes. Other findings include flattening, sclerosis, enlargement, cystic lesions, and bone oedema affecting the articulating surfaces of the two spinous processes. There may be oedema of the interspinous ligament. Gadolinium administration may show enhancement of this area. Rarely there may be epidural cysts or epidural fibrotic masses causing dural compression.[5]
![MRI, STIR sequence, sagittal reconstruction illustrating bone oedema at both the spinous processes of L3-L4 level.[5]](/w/img_auth.php/thumb/8/8d/Baastrup_kissing_spine_bone_oedema_MRI.jpg/301px-Baastrup_kissing_spine_bone_oedema_MRI.jpg)
MRI, STIR sequence, sagittal reconstruction illustrating bone oedema at both the spinous processes of L3-L4 level.[5]
![Lumbar spine X-ray, AP (left image) and lateral (right image) views illustrating close approximation and contact of spinous processes at L4-L5 level with sclerosis and flattening of the articulating surfaces (white arrow).[5]](/w/img_auth.php/thumb/f/f5/Baastrup_kissing_spine_XR.jpg/498px-Baastrup_kissing_spine_XR.jpg)
Lumbar spine X-ray, AP (left image) and lateral (right image) views illustrating close approximation and contact of spinous processes at L4-L5 level with sclerosis and flattening of the articulating surfaces (white arrow).[5]
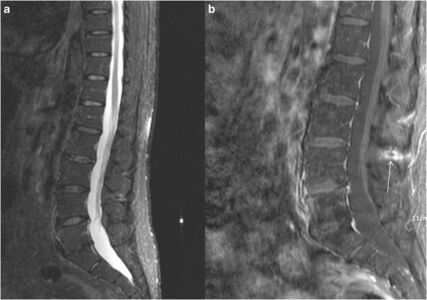
MRI, sagittal reconstruction: STIR sequence (a) illustrating high signal intensity and fat-suppression T1-weighted sequence, post intravenous gadolinium injec
![MRI, STIR sequence, sagittal reconstruction illustrating bone oedema at both the spinous processes of L3-L4 level.[5]](/wiki/File:Baastrup_kissing_spine_bone_oedema_MRI.jpg)
![Lumbar spine X-ray, AP (left image) and lateral (right image) views illustrating close approximation and contact of spinous processes at L4-L5 level with sclerosis and flattening of the articulating surfaces (white arrow).[5]](/wiki/File:Baastrup_kissing_spine_XR.jpg)

Diagnosis

In the appropriate clinical setting and imaging findings, the diagnosis can be confirmed by finding resolution of pain with a diagnostic injection of local anaesthetic under fluoroscopic guidance.[3]
The interspinous soft tissues are supplied by the medial branches of the dorsal ramui. Therefore medial branch diagnostic blocks would be positive, and radiofrequency neurotomy of the medial branches would relieve the pain. There is discussion amongst the Musculoskeletal Medicine community as to whether, if the history fits, should symptomatic interspinous oedema be excluded by the appropriate MRI sequences before embarking on MBBs?
Treatment
Treatment options include NSAIDs, corticosteroid injections, and surgical therapies which include excision of the bursa or osteotomy. There may be additional factors in the patients pain such as facet joint irritation which may need to be addressed.
Injections

Injections are performed at the level of the interspinous ligament and have been used with good therapeutic benefit.[3] There is usually durable fast relief by an interspinous injection of steroid and local anaesthetic. This should ideally be done with imaging guidance to ensure accurate needle positioning. In New Zealand, fluoroscopic guidance is normally used. Ultrasound could theoretically be used as an alternative, however this has not been studied.
The technique used by one Musculoskeletal Physician in New Zealand is as follows:
- Advance a 9 cm 22-gauge spinal needle into the interspinous space using AP and lateral projections.
- Infiltrated 1 mL Omnipaque 300 into the interspinous space to ensure position.
- Infiltrate a mixture of 40 mg Kenacort A and 0.5 mL 0.75% Ropivacaine into the affected interspinous space.
Surgery
Surgery for interspinous oedema is not indicated, and for kissing spines it is often not successful.
Resources
- An open access review of kissing spines is available by Filippiadis et al.[5]
Summary
- The clinical history and examination and imaging findings of traumatic symptomatic lumbar oedema is described along with it’s management
- Interpinous oedema can be asymptomatic, but is more common in symptomatic patients.[Level 5]
- The symptomatic patient is definite about an accident with the pain being closely linked to the inciting event. The pain distribution is quite variable, but the pain intensity is often severe with marked effects on function. There is tenderness in the affected interspinous space.[Level 5]
- For diagnosis the MRI needs to include a coronal T2 fat sat Dixon sequence, and the diagnosis is supported by abolition of pain with image guided injection.[Level 5]
- If looking at doing medial branch blocks, consider first excluding the presence of interspinous oedema on MRI.[Level 5]
- There is usually durable fast relief by an interspinous injection of steroid and LA. [Level 5]
References
- ↑ 1.0 1.1 Bogduk, Nikolai. Clinical and radiological anatomy of the lumbar spine. Chapter 15. Edinburgh: Elsevier/Churchill Livingstone, 2012.
- ↑ 2.0 2.1 2.2 Correspondence with Dr Mike Cleary, Musculoskeletal Medicine Physician
- ↑ 3.0 3.1 3.2 3.3 DePalma et al.. Interspinous bursitis in an athlete. The Journal of bone and joint surgery. British volume 2004. 86:1062-4. PMID: 15446539. DOI.
- ↑ 4.0 4.1 Maes et al.. Lumbar interspinous bursitis (Baastrup disease) in a symptomatic population: prevalence on magnetic resonance imaging. Spine 2008. 33:E211-5. PMID: 18379391. DOI.
- ↑ 5.0 5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 Filippiadis et al.. Baastrup's disease (kissing spines syndrome): a pictorial review. Insights into imaging 2015. 6:123-8. PMID: 25582088. DOI. Full Text.
- ↑ Beks. Kissing spines: fact or fancy?. Acta neurochirurgica 1989. 100:134-5. PMID: 2589119. DOI.
- ↑ Salvarani et al.. Cervical interspinous bursitis in active polymyalgia rheumatica. Annals of the rheumatic diseases 2008. 67:758-61. PMID: 18208867. DOI.
- ↑ Camellino et al.. Interspinous bursitis is common in polymyalgia rheumatica, but is not associated with spinal pain. Arthritis research & therapy 2014. 16:492. PMID: 25435011. DOI. Full Text.
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,

