Lumbar Radicular Pain and Radiculopathy: Difference between revisions
No edit summary |
No edit summary |
||
| Line 4: | Line 4: | ||
==Sensory Deficit Maps with Nerve Block== | ==Sensory Deficit Maps with Nerve Block== | ||
In 1993 Nitta et al looked at dermatome patterns by doing fluoroscopically guided spinal nerve anaesthetic blocks in patients with radicular pain. They found the following sensory deficits. | In 1993 Nitta et al looked at dermatome patterns by doing fluoroscopically guided spinal nerve anaesthetic blocks in patients with radicular pain. They found the following sensory deficits.<ref>{{#pmid:8235861}}</ref> | ||
<gallery widths=250 heights=250> | <gallery widths=250 heights=250> | ||
File:L4 nerve block sensory deficit Nitta.png|L4 block pattern: Extending from the midline of the trunk posteriorly, across the buttock, through the lateral and anterior side of the thigh and the medial side of the leg to the first digit of the foot. | File:L4 nerve block sensory deficit Nitta.png|L4 block pattern: Extending from the midline of the trunk posteriorly, across the buttock, through the lateral and anterior side of the thigh and the medial side of the leg to the first digit of the foot. | ||
Revision as of 15:55, 25 April 2021

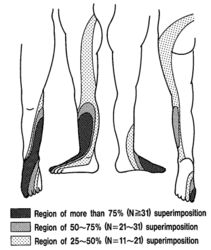
Radicular pain is generated by discharges from a dorsal root or dorsal root ganglion. Inflammation plays an important role as simple compression does not necessarily result in pain. In the lumbar spine, the pain is often described as travelling along the length of the limb in a narrow band two to three inches wide.[1] L4, L5, and S1 pain patterns have significant overlapping pain areas.
Sensory Deficit Maps with Nerve Block
In 1993 Nitta et al looked at dermatome patterns by doing fluoroscopically guided spinal nerve anaesthetic blocks in patients with radicular pain. They found the following sensory deficits.[2]

L4 block pattern: Extending from the midline of the trunk posteriorly, across the buttock, through the lateral and anterior side of the thigh and the medial side of the leg to the first digit of the foot.
L5 block pattern: Extending from the midline of the trunk posteriorly, across the buttock, through the posterior, lateral aspect of the thigh and leg, to the 5th digit of the foot.

S1 block pattern: Extending from the midline of the trunk posteriorly, across the buttock, through the lateral side of the thigh, the lateral side of the leg, and the medial side of the dorsum of the foot to the first digit.
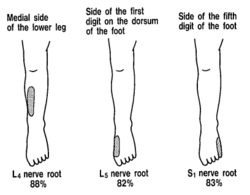
Distinctive regions. L4 is medial side of the lower leg in 88%. L5 is first dorsal digit in 82%. S1 is lateral side of 5th digit in 83%.
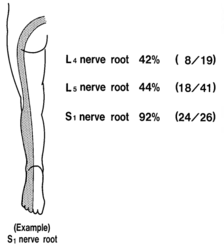
Proportion having band like deficits.





Inadvertent Pain Maps during TFI
Furman et al in 2019 mapped lower limb radicular symptoms based on inadvertent pain patterns during supraneural transforaminal injections, the data is modified in table format below. They confirmed that history and pain charts cannot predict the nerve root level. The buttock is a very common pain referral location across all nerve roots, while pain in the thigh and leg frequently follows dermatomal distributions. A significant limitation of the study is that injectate in transforaminal injections frequently traverses segment levels.[3]
| Nerve Root | L3 | L4 | L5 | S1 |
|---|---|---|---|---|
| Buttock | 45% | 43% | 62% | 64% |
| Groin | 0% | 3% | 0% | 0% |
| Anterior Thigh | 27% | 29% | 12% | 0% |
| Posterior Thigh | 36% | 25% | 59% | 36% |
| Medial Thigh | 18% | 11% | 3% | 0% |
| Lateral Thigh | 0% | 14% | 9% | 0% |
| Knee | 9% | 7% | 6% | 9% |
| Anterior Leg | 0% | 14% | 3% | 0% |
| Posterior Leg | 18% | 18% | 50% | 45% |
| Medial Leg | 0% | 7% | 6% | 0% |
| Lateral Leg | 9% | 14% | 24% | 0% |
| Foot | 0% | 3% | 0% | 0% |
References
- ↑ Bogduk. On the definitions and physiology of back pain, referred pain, and radicular pain. Pain 2009. 147:17-9. PMID: 19762151. DOI.
- ↑ Nitta et al.. Study on dermatomes by means of selective lumbar spinal nerve block. Spine 1993. 18:1782-6. PMID: 8235861. DOI.
- ↑ Furman & Johnson. Induced lumbosacral radicular symptom referral patterns: a descriptive study. The spine journal : official journal of the North American Spine Society 2019. 19:163-170. PMID: 29800710. DOI.
Literature Review
 Literature Review
Literature Review
- Reviews from the last 7 years: review articles, free review articles, systematic reviews, meta-analyses, NCBI Bookshelf
- Articles from all years: PubMed search, Google Scholar search.
- TRIP Database: clinical publications about evidence-based medicine.
- Other Wikis: Radiopaedia, Wikipedia Search, Wikipedia I Feel Lucky, Orthobullets,

