Sacroiliac Joint: Difference between revisions
No edit summary |
No edit summary |
||
| Line 41: | Line 41: | ||
Sacral counternutation: posterior tilt of the superior sacrum. Limited primarily by the LPSL, and also by the thoracolumbar fascia and latissimus dorsi. | Sacral counternutation: posterior tilt of the superior sacrum. Limited primarily by the LPSL, and also by the thoracolumbar fascia and latissimus dorsi. | ||
The SIJ has a self-locking mechanism. Form-closure refers to the vertical support of load, and force-closure refers to the horizontal support of load. | |||
==Gallery== | ==Gallery== | ||
Revision as of 18:00, 7 September 2020
The sacroiliac joint, formed at the junction of the bilateral iliac wings with the sacrum, is a common source of acute and chronic low back pain. It has a complex structure.
Bony and Cartilaginous Structures
The sacroiliac joint is around 1-2mm wide and is formed within S1, S2, and S3. The concave sacral surface joins with the convex ilium surface. The joint has an interlocking mechanism due to an irregular sacral surface, which gives the joint the highest friction coefficient in the whole body. The joint space decreases with age, and becomes stiffer and less effective at shock absorption.
The sacroiliac joint has mostly been described as a diarthrodial synovial joint. However it has also been reported as being an amphiarthrosis, and this appearance is more common with age. The interosseous portion differentiates it from other diarthrodial joints.
Reports disagree as to the cartilage lining of the joint, with some authors concluding that the iliac side is lined by fibrocartilage and the sacral side lined by hyaline cartilage. Other authors state there is a mixture on both sides. The sacral side is 2-3 times thicker than the iliac side, and the sacral side is even thicker in women. The articular surfaces display degenerative changes such as erosions and cortical irregularities from as young as 20 years old, more prominent on the iliac side.
The anterior aspect of the joint is a synovial joint, while the posterior aspect is more of a syndesmosis with multiple myoligamentous attachments. Joint stability is provided by multiple ligaments and muscles. The gluteal muscles form some of the connections between the pelvis and hip, and can be painful in those with sacroiliac joint dysfunction.
Ligaments
Several ligaments help maintain stability and reduce the mechanical stress applied through the joint. The capsule is often indistinguishable from the surrounding ligaments. The sacroiliac joint consists of intrinsic (capsular) and extrinsic (accessory) ligaments. The intrinsic ligaments include the anterior sacroiliac ligament (ASL), the interosseous sacroiliac ligament (ISL), the posterior sacroiliac ligament (PSL), and the long posterior sacroiliac ligament (LPSL). The extrinsic ligaments include the iliolumbar ligament (ILL), the sacrotuberous ligament (STL), and the sacrospinous ligament (SSL).
- Anterior sacroiliac ligament
- This thin ligament is a thickening of the anterior and inferior aspects of the joint capsule. It passes from the anterior aspect of the sacrum, crosses the SIJ, and inserts on the anteromedial aspect of the ilium near the articular margin.
- Posterior sacroiliac ligamentous complex
- The fibres merge with other ligamentous structures. The LPSL attaches to the inferior lateral sacral crest. The PSL attaches to variable sites on the sacrum. The ISL is deep to the PSL. The LPSL is lateral to the PSL.
- Interosseous sacroiliac ligament
- This fills the syndesmotic joint space as the deepest layer posteriorly. It is only present in the cranial joint aspect. It attaches to the iliac tuberosity.
- Posterior sacroiliac ligament
- Found posterior to the sacroiliac joint. There are two groups, the cranial and caudal groups. The cranial group runs from the lateral edge of the posterior aspect of the sacral and attaches to the ridge on the ilium. Superiorly it merges with the ASL. The caudal group is the true PSL, and passes from the iliac tuberosity to the first sacral segment, lateral sacral tubercle, and the base of the articular process. Some fibres attach to the PSIS.
- Long posterior sacroiliac ligament
- Runs from the PSIS to the third or fourth lateral sacral tubercles. It is penetrated by S2-S4 dorsal sacral rami. The LPSL is under tension during SIJ counternutation (posterior rotation), and is slack during nutation. It is closely approximated with the erector spinae muscles, the posterior layer of the thoracolumbar fascia, and parts of the sacrotuberous ligament. It forms a functional link between legs, spine, and arms. The medial cluneal nerves can be associated with it. It is a potential pain generator.
- Iliolumbar ligament
- Runs from the transverse process of L5 to the posterior part of the iliac crest. It may arise from L4.
- Sacrospinous and sacrotuberous ligaments
- These two ligaments prevent sacral tilting. the SSL runs from the anterolateral aspects of the caudal 2 sacral segments, and the first coccygeal segment, along to the ischial spine. The STL runs from the PSIS to the iliac border to the caudal sacral and coccygeal edge, and also to the lateral sacral crest, and inserts on the ischial tuberosity. There are various muscular and fascial attachments as well (erector spinae, piriformis, gluteus maximus, biceps femoris, and thoracolumbar fascia). The SSL is the main ligamentous structure that restricted sacral nutation.
Innervation
The anterior aspect of the joint is innervated by L4-S2, sometimes L3, and the sacral plexus. The posterior aspect of the joint is supplied by a plexus that is formed by the lateral branches of the posterior rami of L5 to S4. The posterior innervation varies from person to person, side to side, and level to level.The superior gluteal nerve may contribute to both anterior and posterior innervation.
Biomechanics
It provides pelvic stabilisation through the transmission and dissipation of forces from the trunk down to he lower extremeties.
The unique joint shape and irregularities of the joint surface causes high frictional resistance limiting joint movement, which is 1–3° in all three axes.
Injury can be caused by axial loading followed by abrupt axial rotation. Repetitive torsional forces can cause inflammation. Pathology can be present in any combination of the sacroiliac joint synovium, capsule, or ligaments, which may lead to hypo- or hypermobility.
Sacral nutation: anterior tilt of the superior sacrum. Limited primarily by the SSL
Sacral counternutation: posterior tilt of the superior sacrum. Limited primarily by the LPSL, and also by the thoracolumbar fascia and latissimus dorsi.
The SIJ has a self-locking mechanism. Form-closure refers to the vertical support of load, and force-closure refers to the horizontal support of load.
Gallery


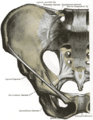
Bony landmarks

Posterior ligaments

Posterior ligaments
Anterior ligaments





Recommended Articles
- Review by Poilliot et al, free access [1]

