⬤
Cervical Spine Injuries (Acute): Difference between revisions
From WikiMSK
No edit summary |
No edit summary |
||
| Line 43: | Line 43: | ||
* Sub-classification: Type I (above transverse ligament), type II (odontoid base), type III (extension to body of C2) | * Sub-classification: Type I (above transverse ligament), type II (odontoid base), type III (extension to body of C2) | ||
* Stability: Types II, III unstable. | * Stability: Types II, III unstable. | ||
<gallery> | |||
File:Atlantoaxial dislocation.png|Atlantoaxial dislocation | |||
File:Atlanto-occipital dislocation.png|Atlanto-occipital dislocation | |||
File:Wedge.png|Wedge fracture | |||
File:Flexion teardrop.png|Flexion teardrop fracture | |||
File:Clay shoveler.png|Clay shoveler fracture | |||
File:Facet dislocation.png|Facet dislocation | |||
File:Dens fractures.png|Odontoid process fracture | |||
</gallery> | |||
== Flexion/Rotation Injuries == | == Flexion/Rotation Injuries == | ||
| Line 55: | Line 64: | ||
* Flexion and rotation centered around single facet results in contralateral facet dislocation. | * Flexion and rotation centered around single facet results in contralateral facet dislocation. | ||
* Imaging: AP radiograph shows spinous processes above dislocation displaced from midline, lateral radiograph shows anterior displacement of lower vertebra (less than ½ AP diameter of vertebral body). | * Imaging: AP radiograph shows spinous processes above dislocation displaced from midline, lateral radiograph shows anterior displacement of lower vertebra (less than ½ AP diameter of vertebral body). | ||
<gallery> | |||
File:Unilateral facet.png|Unilateral facet dislocation | |||
</gallery> | |||
== Extension Injuries == | == Extension Injuries == | ||
| Line 75: | Line 87: | ||
* Complications: Central cord syndrome | * Complications: Central cord syndrome | ||
* Stability: Unstable in extension | * Stability: Unstable in extension | ||
<gallery> | |||
File:Posterior arch fracture.png|Posterior neural arch fracture | |||
File:Hangman-fracture.png|Hangman's fracture | |||
File:Extension teardrop.png|Extension-teardrop fracture | |||
</gallery> | |||
== Vertical compression == | == Vertical compression == | ||
| Line 90: | Line 107: | ||
* Imaging: Widening of predental space. Open-mouth odontoid view may reveal bilateral offset distance of >7mm between lateral masses of C1/C2. | * Imaging: Widening of predental space. Open-mouth odontoid view may reveal bilateral offset distance of >7mm between lateral masses of C1/C2. | ||
* Stability: Unstable | * Stability: Unstable | ||
<gallery> | |||
File:Burst.png|Burst fracture | |||
File:Jefferson.png|Jefferson fracture | |||
</gallery> | |||
== References == | == References == | ||
Revision as of 06:56, 7 May 2022

Flexion Injuries
C1/C2
- Atlanto-occipital dislocation , atlantoaxial dislocations , potentially associated with odontoid fracture.
- Imaging: Basion-dens interval (BDI) >10mm,
- Stability: Unstable.
Wedge fracture
- Stretch on strong nuchal ligament transmits force to vertebral body.
- Stability: Generally stable unless >50% compression or multiple contiguous.
Flexion-teardrop fracture
- Severe flexion force, avulsion of fragment of anterior/inferior portion of vertebral body.
- Stability: Unstable, involves anterior/posterior ligamentous disruptions.
Clay shoveler’s fracture
- Oblique fracture of spinous process of lower cervical spine.
- Stability: Stable
Subluxation
- Pure ligamentous injury without associated fracture.
- Imaging: Widening of interspinous and intervertebral spaces on lateral.
- Stability: Potentially unstable.
Bilateral facet dislocation
- Anterior displacement of spine above level of injury caused by dislocation of upper inferior facet from lower superior facet.
- Imaging: Anterior displacement greater than ½ AP diameter of vertebral body.
- Stability: Unstable
Odontoid process fracture
- Head trauma with shear force directed at odontoid.
- Sub-classification: Type I (above transverse ligament), type II (odontoid base), type III (extension to body of C2)
- Stability: Types II, III unstable.
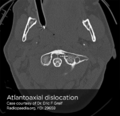
Atlantoaxial dislocation

Atlanto-occipital dislocation
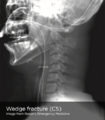
Wedge fracture

Flexion teardrop fracture

Clay shoveler fracture

Facet dislocation

Odontoid process fracture






Flexion/Rotation Injuries
Rotary atlantoaxial dislocation
- Imaging: Open-mouth odontoid, asymmetric lateral masses of C1.
- Stability: Unstable
Unilateral facet dislocation
- Flexion and rotation centered around single facet results in contralateral facet dislocation.
- Imaging: AP radiograph shows spinous processes above dislocation displaced from midline, lateral radiograph shows anterior displacement of lower vertebra (less than ½ AP diameter of vertebral body).

Unilateral facet dislocation

Extension Injuries
Posterior neural arch fracture (C1)
- Forced extension causes compressive force on posterior elements of C1 between occiput and C2.
- Stability: Unstable
Hangman’s fracture (spondylolysis C2)
- Abrupt deceleration causes fracture of bilateral pedicles of C2, potentially with associated subluxation. Rarely associated with SCI due to large diameter of neural canal at C2.
- Imaging: May be associated with retropharyngeal space edema.
- Stability: Unstable
Extension-teardrop fracture
- Abrupt extension (ex. diving) results in stretch along anterior longitudinal ligament with avulsion of anterior/inferior fragment of vertebral body (usually C5-C7).
- Imaging: May be radiographically similar to flexion-teardrop fracture.
- Complications: Central cord syndrome
- Stability: Unstable in extension

Posterior neural arch fracture

Hangman's fracture
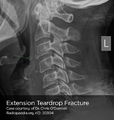
Extension-teardrop fracture



Vertical compression
Burst fracture
- Force applied from above or below causes transmission of force to intervertebral disc and vertebral body.
- Imaging: Comminuted vertebral body, >40% compression of anterior vertebral body.
- Complications: Fracture fragments may impinge on spinal cord.
- Stability: Stable
Jefferson fracture (C1)
- Vertical force transmitted from occipital condyles to superior articular facets of atlas, resulting in fractures of anterior and posterior arches.
- Imaging: Widening of predental space. Open-mouth odontoid view may reveal bilateral offset distance of >7mm between lateral masses of C1/C2.
- Stability: Unstable

Burst fracture
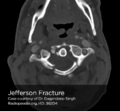
Jefferson fracture


References
- MD RK, MD BED, CAQ-SM KHM, MD WF. Emergency Department Evaluation and Treatment of Cervical Spine Injuries. Emergency Medicine Clinics of NA. 2015;33(2):241-282. doi:10.1016/j.emc.2014.12.002.
- Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin Orthop Relat Res. 1984;(189):65-76.
- Munera F, Rivas LA, Nunez DB, Quencer RM. Imaging evaluation of adult spinal injuries: emphasis on multidetector CT in cervical spine trauma. Radiology. 2012;263(3):645-660. doi:10.1148/radiol.12110526.

