Tibiotalar Joint (Talocrural Joint): Difference between revisions
mNo edit summary |
No edit summary |
||
| Line 4: | Line 4: | ||
|name= | |name= | ||
|synonym=Ankle joint, talocrural joint, tibiotalar joint | |synonym=Ankle joint, talocrural joint, tibiotalar joint | ||
|type=Diarthrodial hinge joint | |type=Diarthrodial uniaxial hinge joint | ||
|bones= | |bones= | ||
|ligaments=Syndesmosis, medial collateral ligaments, lateral collateral ligaments | |ligaments=Syndesmosis, medial collateral ligaments, lateral collateral ligaments | ||
| Line 10: | Line 10: | ||
|innervation=tibial nerve, deep peroneal nerve | |innervation=tibial nerve, deep peroneal nerve | ||
|vasculature=anterior and posterior tibial arteries, peroneal artery | |vasculature=anterior and posterior tibial arteries, peroneal artery | ||
|rom= | |rom=10° to 20° of dorsiflexion, 40° to 55° of plantarflexion | ||
|volume= | |volume= | ||
|conditions= | |conditions= | ||
}} | }} | ||
The tibiotalar joint, also known as the ankle joint or talocrural joint, is formed by the junction between the distal tibia and fibula and the talus. | |||
The tibiotalar joint, also known as the ankle joint or talocrural joint, is formed by the junction between the distal tibia and fibula and the talus. It has evolved for stability rather than mobility. | |||
==Bony Anatomy== | ==Bony Anatomy== | ||
The tibial-talar aspect bears the load. A mortise is formed by the distal aspects of the tibia and fibula, and the trochlea of the talus fits into this. The malleoli of the tibia and fibula constrain the talus forming a hinge joint providing plantarflexion and dorsiflexion of the foot. | The tibial-talar aspect bears the load. A mortise is formed by the distal aspects of the tibia and fibula, and the trochlea of the talus fits into this. The malleoli of the tibia and fibula constrain the talus forming a hinge joint providing plantarflexion and dorsiflexion of the foot. | ||
The hinge terminology is somewhat of a simplification. The trochlea surface is cone-shaped and it has an oblique rotation axis. The talus is widest anteriorly, leading to the joint being most stable in a position of dorsiflexion. | The hinge terminology is somewhat of a simplification. The trochlea surface is cone-shaped and it has an oblique rotation axis. The talus is widest anteriorly, leading to the joint being most stable in a position of dorsiflexion, called a "close packed" position. | ||
Stability is provided by the joint geometry (especially in the stance phase of the [[gait]]) and the soft tissue structures. | Stability is provided by the joint geometry (especially in the stance phase of the [[gait]]) and the soft tissue structures. | ||
| Line 28: | Line 29: | ||
There are three groups of ligaments that provide stability | There are three groups of ligaments that provide stability | ||
* Tibiofibular syndemosis. This limits motion between the tibia and fibula. There are three parts - the anterior tibiofibular ligament, the posterior tibiofibular ligament, and the interosseous tibiofibular ligament | * '''Tibiofibular syndemosis'''. This limits motion between the tibia and fibula. There are three parts - the anterior tibiofibular ligament, the posterior tibiofibular ligament, and the interosseous tibiofibular ligament | ||
* Medial collateral ligaments (deltoid ligaments). These resist eversion and valgus stresses. It is fan shaped and has anterior and posterior tibiotalar ligaments, the tibionavicular ligament, and the tibiocalcaneal ligament | * '''Medial collateral ligaments''' (deltoid ligaments). These resist eversion and valgus stresses. It is fan shaped and has anterior and posterior tibiotalar ligaments, the tibionavicular ligament, and the tibiocalcaneal ligament | ||
* Lateral collateral ligaments. These protect against inversion of the joint limiting varus stresses and reduce rotation. They are the anterior and posterior talofibular ligaments and the calcaneofibular ligament. The lateral ligaments are frequently injured during inversion injuries. The calcaneofibular ligament is the only direct soft tissue connection between the tibiotalar and [[Talocalcaneal Joint (Subtalar Joint)|subtalar joint]]. | * '''Lateral collateral ligaments'''. These protect against inversion of the joint limiting varus stresses and reduce rotation. They are the anterior and posterior talofibular ligaments and the calcaneofibular ligament. The lateral ligaments are frequently injured during inversion injuries. The calcaneofibular ligament is the only direct soft tissue connection between the tibiotalar and [[Talocalcaneal Joint (Subtalar Joint)|subtalar joint]]. | ||
<gallery mode="packed" heights="250"> | <gallery mode="packed" heights="250"> | ||
File:Lateral collateral ligament of ankle.png|Lateral collateral ligament | File:Lateral collateral ligament of ankle.png|Lateral collateral ligament | ||
| Line 36: | Line 37: | ||
File:Deltoid ligament deep layer.jpg|Deltoid ligament deep layer | File:Deltoid ligament deep layer.jpg|Deltoid ligament deep layer | ||
</gallery> | </gallery> | ||
== Movement == | |||
The two movements are dorsiflexion and plantarflexion. The axis of rotation for the ankle joint is a line that runs slightly obliquely i.e. not in line with the body. The axis can be estimated by placing your fingers on each of the malleoli. The lateral portion (lateral malleolus) is posteriorly and inferiorly located to the medial portion (medial malleolus) | |||
The axis is approximately at 10° with the horizontal medial-lateral axis in the coronal plane, and approximately at 6° with the horizontal medial-lateral axis in the transverse plane. This obliquity is minor and so in most situations the joint is considered to function in the sagittal plane alone. | |||
There is a wide range of normal. With goniometric measurements the range is 10° to 20° of dorsiflexion and 40° to 55° of plantarflexion. The joints of the midfoot contribute 10% to 41% of plantarflexion from neutral to 30° plantarflexion. | |||
== References == | |||
* Basic Biomechanics of the Musculoskeletal System - Nordin 4th edition 2012 | |||
[[Category:Foot and Ankle Anatomy]] | [[Category:Foot and Ankle Anatomy]] | ||
Revision as of 10:06, 18 July 2021
{{{{{quality}}}}}
| Tibiotalar Joint (Talocrural Joint) | |
|---|---|
| Synonym | Ankle joint, talocrural joint, tibiotalar joint |
| Primary Type | Diarthrodial uniaxial hinge joint"Diarthrodial uniaxial hinge joint" is not in the list (Synovial Joint, Cartilaginous Joint, Fibrous Joint, Compound Joint) of allowed values for the "Has joint type" property. |
| Secondary Type | |
| Bones | |
| Ligaments | Syndesmosis, medial collateral ligaments, lateral collateral ligaments |
| Muscles | |
| Innervation | tibial nerve, deep peroneal nerve |
| Vasculature | anterior and posterior tibial arteries, peroneal artery |
| ROM | 10° to 20° of dorsiflexion, 40° to 55° of plantarflexion |
| Volume | |
| Conditions | |
The tibiotalar joint, also known as the ankle joint or talocrural joint, is formed by the junction between the distal tibia and fibula and the talus. It has evolved for stability rather than mobility.
Bony Anatomy
The tibial-talar aspect bears the load. A mortise is formed by the distal aspects of the tibia and fibula, and the trochlea of the talus fits into this. The malleoli of the tibia and fibula constrain the talus forming a hinge joint providing plantarflexion and dorsiflexion of the foot.
The hinge terminology is somewhat of a simplification. The trochlea surface is cone-shaped and it has an oblique rotation axis. The talus is widest anteriorly, leading to the joint being most stable in a position of dorsiflexion, called a "close packed" position.
Stability is provided by the joint geometry (especially in the stance phase of the gait) and the soft tissue structures.
The joint has a thin capsule that attaches to the tibia, malleoli, and talus.
Ligaments
There are three groups of ligaments that provide stability
- Tibiofibular syndemosis. This limits motion between the tibia and fibula. There are three parts - the anterior tibiofibular ligament, the posterior tibiofibular ligament, and the interosseous tibiofibular ligament
- Medial collateral ligaments (deltoid ligaments). These resist eversion and valgus stresses. It is fan shaped and has anterior and posterior tibiotalar ligaments, the tibionavicular ligament, and the tibiocalcaneal ligament
- Lateral collateral ligaments. These protect against inversion of the joint limiting varus stresses and reduce rotation. They are the anterior and posterior talofibular ligaments and the calcaneofibular ligament. The lateral ligaments are frequently injured during inversion injuries. The calcaneofibular ligament is the only direct soft tissue connection between the tibiotalar and subtalar joint.
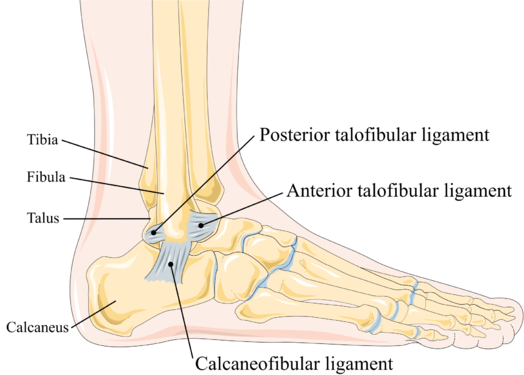
Lateral collateral ligament
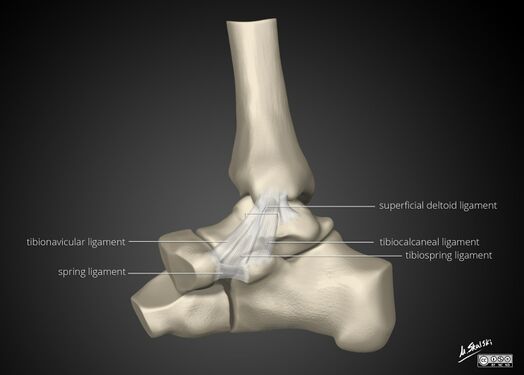
Deltoid ligament superficial layer

Deltoid ligament deep layer



Movement
The two movements are dorsiflexion and plantarflexion. The axis of rotation for the ankle joint is a line that runs slightly obliquely i.e. not in line with the body. The axis can be estimated by placing your fingers on each of the malleoli. The lateral portion (lateral malleolus) is posteriorly and inferiorly located to the medial portion (medial malleolus)
The axis is approximately at 10° with the horizontal medial-lateral axis in the coronal plane, and approximately at 6° with the horizontal medial-lateral axis in the transverse plane. This obliquity is minor and so in most situations the joint is considered to function in the sagittal plane alone.
There is a wide range of normal. With goniometric measurements the range is 10° to 20° of dorsiflexion and 40° to 55° of plantarflexion. The joints of the midfoot contribute 10% to 41% of plantarflexion from neutral to 30° plantarflexion.
References
- Basic Biomechanics of the Musculoskeletal System - Nordin 4th edition 2012

